Fung Alastair, Horton Susan, Zabih Veda, Denburg Avram, Gupta Sumit
Pediatrics and Child Health, Winnipeg Children's Hospital, Winnipeg, Manitoba, Canada.
School of Public Health and Health Systems, University of Waterloo, Waterloo, Ontario, Canada.
BMJ Glob Health. 2019 Oct 31;4(5):e001825. doi: 10.1136/bmjgh-2019-001825. eCollection 2019.
A major barrier to improving childhood cancer survival is the perception that paediatric oncology services are too costly for low-income and middle-income country (LMIC) health systems. We conducted a systematic review to synthesise existing evidence on the costs and cost-effectiveness of treating childhood cancers in LMICs.
We searched multiple databases from their inception to March 2019. All studies reporting costs or cost-effectiveness of treating any childhood cancer in an LMIC were included. We appraised included articles using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist. Where possible, we extracted or calculated the cost per disability-adjusted life year (DALY) averted using reported survival and country-specific life expectancy. Cost/DALY averted was compared with per capita gross domestic product (GDP) as per WHO-Choosing Interventions that are Cost-Effective guidelines to determine cost-effectiveness.
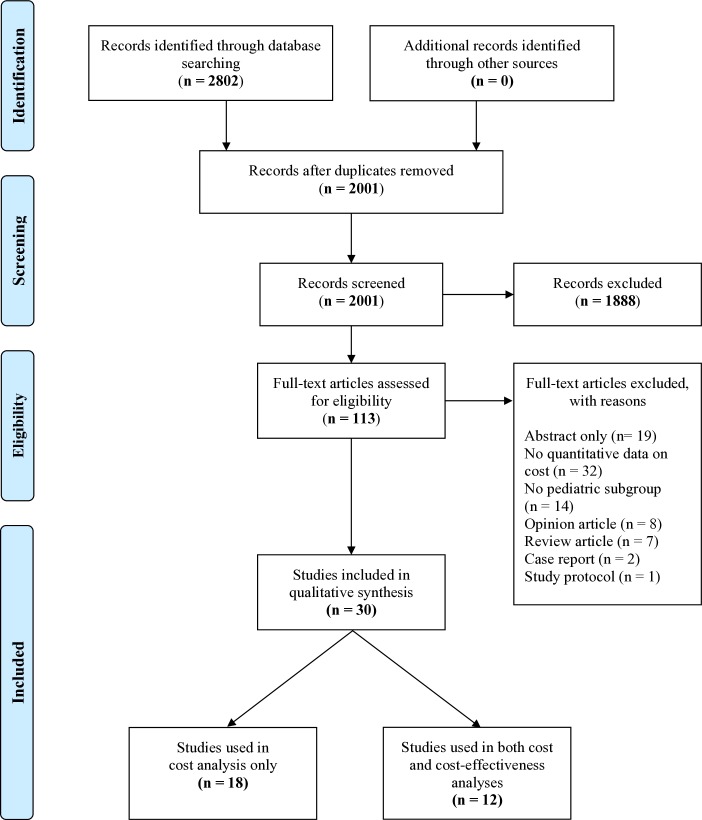
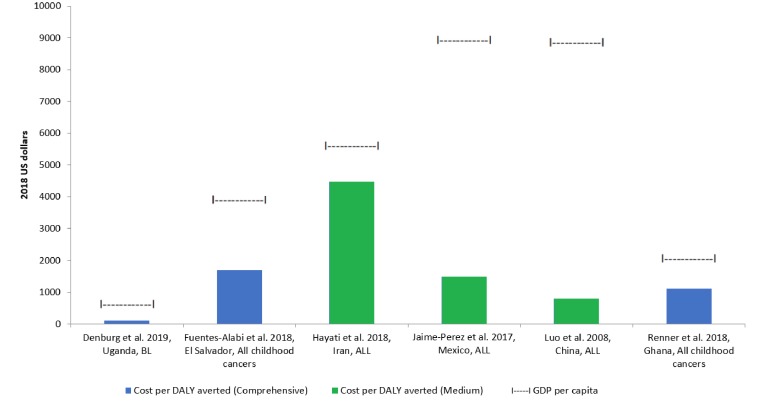
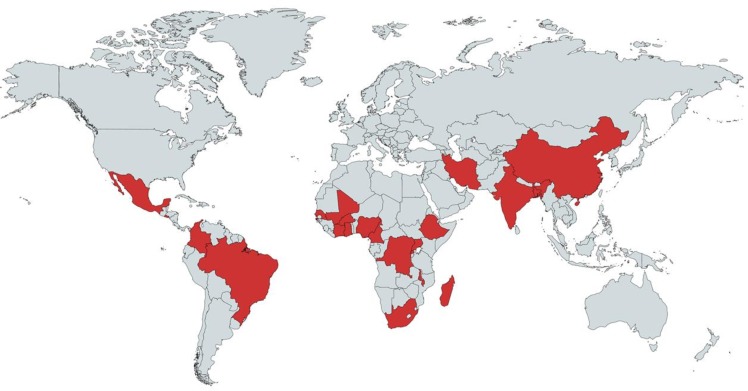
Of 2802 studies identified, 30 met inclusion criteria. Studies represented 22 countries and nine different malignancies. The most commonly studied cancers were acute lymphoblastic leukaemia (n=10), Burkitt lymphoma (n=4) and Wilms tumour (n=3). The median CHEERS checklist score was 18 of 24. Many studies omitted key cost inputs. Notably, only 11 studies included healthcare worker salaries. Cost/DALY averted was extracted or calculated for 12 studies and ranged from US$22 to US$4475, although the lower-end costs were primarily from studies that omitted key cost components. In all 12, cost/DALY averted through treatment was substantially less than country per capita GDP, and therefore considered very cost-effective.
Many included studies did not account for key cost inputs, thus underestimating true treatment costs. Costs/DALY averted were nonetheless substantially lower than per capita GDP, suggesting that even if all relevant inputs are included, LMIC childhood cancer treatment is consistently very cost-effective. While additional rigorous economic evaluations are required, our results can inform the development of LMIC national childhood cancer strategies.
改善儿童癌症生存率的一个主要障碍是,人们认为儿科肿瘤服务对于低收入和中等收入国家(LMIC)的卫生系统而言成本过高。我们进行了一项系统综述,以综合现有关于低收入和中等收入国家儿童癌症治疗成本及成本效益的证据。
我们检索了多个数据库,时间跨度从其创建至2019年3月。纳入所有报告低收入和中等收入国家任何儿童癌症治疗成本或成本效益的研究。我们使用《卫生经济评估报告标准合并清单》(CHEERS)对纳入的文章进行评估。在可能的情况下,我们利用报告的生存率和特定国家的预期寿命,提取或计算避免每例伤残调整生命年(DALY)的成本。根据世界卫生组织《选择具有成本效益的干预措施》指南,将避免的成本/ DALY与人均国内生产总值(GDP)进行比较,以确定成本效益。
在确定的2802项研究中,30项符合纳入标准。这些研究涵盖22个国家和9种不同的恶性肿瘤。研究最多的癌症是急性淋巴细胞白血病(n = 10)、伯基特淋巴瘤(n = 4)和肾母细胞瘤(n = 3)。CHEERS清单的中位数分数为24分中的18分。许多研究遗漏了关键的成本投入。值得注意的是,只有11项研究纳入了医护人员的工资。对12项研究提取或计算了避免的成本/ DALY,范围从22美元到4475美元,尽管低端成本主要来自遗漏关键成本组成部分的研究。在所有12项研究中,通过治疗避免的成本/ DALY远低于国家人均GDP,因此被认为具有很高的成本效益。
许多纳入的研究没有考虑关键的成本投入,从而低估了实际治疗成本。然而,避免的成本/ DALY仍远低于人均GDP,这表明即使纳入所有相关投入,低收入和中等收入国家的儿童癌症治疗始终具有很高的成本效益。虽然需要进行更多严格的经济评估,但我们的结果可为低收入和中等收入国家制定国家儿童癌症战略提供参考。