Division of Pulmonary, Allergy and Critical Care Medicine, Department of Medicine, Duke University Medical Center, Durham, NC, USA.
Interventional Pulmonology, Division of Pulmonary & Critical Care Medicine, Duke University Health System, Duke Cancer Center Raleigh, 3404 Wake Forest Road, Suite 303, Raleigh, NC, 27609, USA.
BMC Pulm Med. 2019 Nov 21;19(1):219. doi: 10.1186/s12890-019-0987-3.
Malignant central airway obstruction (CAO) occurs in approximately 20-30% of patients with lung cancer and is associated with debilitating symptoms and poor prognosis. Multimodality therapeutic bronchoscopy can relieve malignant CAO, though carries risk. Evidence to guide clinicians regarding which patients may benefit from such interventions is sparse. We aimed to assess the clinical and radiographic predictors associated with therapeutic bronchoscopy success in relieving malignant CAO.
We reviewed all cases of therapeutic bronchoscopy performed for malignant CAO at our institution from January 2010-February 2017. Therapeutic bronchoscopy success was defined as establishing airway patency of > 50%. Patient demographics and baseline characteristics, oncology history, degree of airway obstruction, procedural interventions, and complications were compared between successful and unsuccessful groups. Univariate and multivariate logistic regression identified the significant clinical and radiographic predictors for therapeutic success. The corresponding simple and conditional odds ratio were calculated. A time-to-event analysis with Kaplan-Meier plots was performed to estimate overall survival.
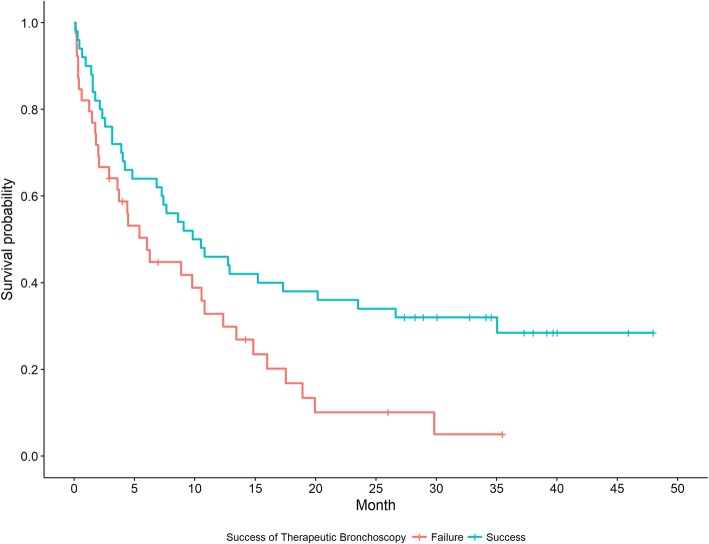
During the study period, 301 therapeutic bronchoscopies were performed; 44 (14.6%) were considered unsuccessful. Factors associated with success included never vs current smoking status (OR 5.36, 95% CI:1.45-19.74, p = 0.010), patent distal airway on CT imaging (OR 15.11, 95% CI:2.98-45.83, p < 0.0001) and patent distal airway visualized during bronchoscopy (OR 10.77, 95% CI:3.63-31.95, p < 0.001) in univariate analysis. Along with patent distal airway on CT imaging, increased time from radiographic finding to therapeutic bronchoscopy was associated with lower odds of success in multivariate analysis (OR 0.96, 95% CI:0.92-1.00, p = 0.048). Median survival was longer in the successful group (10.2 months, 95% CI:4.8-20.2) compared to the unsuccessful group (6.1 months, 95% CI:2.1-10.8, log rank p = 0.015).
Predictors associated with successful therapeutic bronchoscopy for malignant CAO include distal patent airway visualized on CT scan and during bronchoscopy. Odds of success are higher in non-smokers, and with decreased time from radiographic finding of CAO to intervention.
恶性中央气道阻塞(CAO)发生在约 20-30%的肺癌患者中,与衰弱的症状和不良预后有关。多模式治疗性支气管镜检查可以缓解恶性 CAO,但存在风险。指导临床医生哪些患者可能受益于此类干预的证据很少。我们旨在评估与治疗性支气管镜检查缓解恶性 CAO 成功相关的临床和影像学预测因素。
我们回顾了 2010 年 1 月至 2017 年 2 月在我们机构进行的所有治疗性支气管镜检查治疗恶性 CAO 的病例。治疗性支气管镜检查成功定义为气道通畅性>50%。比较成功组和不成功组之间的患者人口统计学和基线特征、肿瘤学史、气道阻塞程度、程序干预和并发症。单变量和多变量逻辑回归确定了治疗成功的显著临床和影像学预测因素。计算了相应的简单和条件优势比。通过 Kaplan-Meier 图进行时间事件分析以估计总生存率。
在研究期间,进行了 301 次治疗性支气管镜检查;44 次(14.6%)被认为不成功。与成功相关的因素包括从不吸烟与当前吸烟状态(OR 5.36,95%CI:1.45-19.74,p=0.010)、CT 成像上的通畅远端气道(OR 15.11,95%CI:2.98-45.83,p<0.0001)和支气管镜检查期间可见的通畅远端气道(OR 10.77,95%CI:3.63-31.95,p<0.001)。在单变量分析中,CT 成像上通畅的远端气道与更高的生存时间相关,这与多变量分析中成功的可能性较低相关(OR 0.96,95%CI:0.92-1.00,p=0.048)。与不成功组相比(6.1 个月,95%CI:2.1-10.8,对数秩 p=0.015),成功组的中位生存时间更长(10.2 个月,95%CI:4.8-20.2)。
与恶性 CAO 的治疗性支气管镜检查成功相关的预测因素包括 CT 扫描和支气管镜检查中可见的远端通畅气道。在非吸烟者和从 CAO 的影像学发现到干预的时间减少时,成功的可能性更高。