Center for Outcomes Research and Evaluation, Yale New Haven Hospital, New Haven, Connecticut.
Section of Cardiovascular Medicine, Department of Internal Medicine, Yale School of Medicine, New Haven, Connecticut.
JAMA Netw Open. 2019 Nov 1;2(11):e1916021. doi: 10.1001/jamanetworkopen.2019.16021.
Determining the association of contrast volume during percutaneous coronary intervention (PCI) with the risk of acute kidney injury (AKI) is important for optimizing PCI safety.
To quantify how the risk of AKI is associated with contrast volume, accounting for the possibility of nonlinearity and heterogeneity among different baseline risks.
DESIGN, SETTING, AND PARTICIPANTS: This prognostic study used data from the American College of Cardiology National Cardiovascular Data Registry CathPCI Registry for 1694 US hospitals. Derivation analysis included 2 076 694 individuals who underwent PCI from July 1, 2011, to June 30, 2015. Validation analysis included 961 863 individuals who underwent PCI from July 1, 2015, to March 31, 2017. Data analysis took place from July 2018 to May 2019.
Contrast volume during PCI.
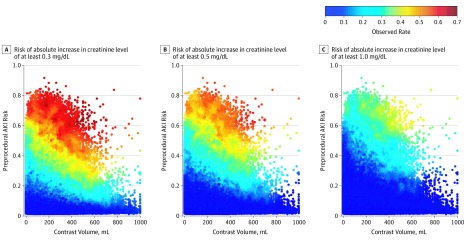
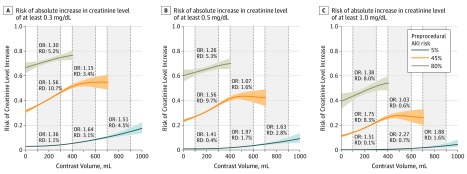
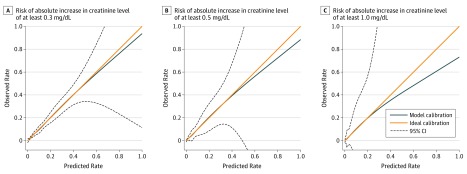
Acute kidney injury was defined using 3 thresholds for preprocedure to postprocedure creatinine level increase (ie, ≥0.3 mg/dL, ≥0.5 mg/dL, and ≥1.0 mg/dL). A model quantifying the association of contrast volume with AKI was developed, and the existence of nonlinearity and heterogeneity were examined by likelihood ratio tests. The model was derived in the training set (a random 50% of the derivation cohort), and performance was evaluated in the test set (the remaining 50% of the derivation cohort) and an independent validation set by area under the receiver operating characteristic curve (AUC) and calibration slope of observed vs predicted risks.
The 2 076 694 patients in the derivation set had a mean (SD) age of 65.1 (12.1) years, and 662 525 (31.9%) were women; 133 306 (6.4%) had creatinine level increases of at least 0.3 mg/dL, 66 626 (3.2%) had creatinine level increases of at least 0.5 mg/dL, and 28 378 (1.4%) had creatinine level increases of at least 1.0 mg/dL. In the validation set of 961 843 patients (mean [SD] age, 65.7 [12.1] years; 305 577 [31.8%] women), these rates were 62 913 (6.5%), 34 229 (3.6%), and 15 555 (1.6%), respectively. The association of contrast volume and AKI risk was nonlinear (χ226 = 1436.2; P < .001) and varied by preprocedural risk (χ220 = 105.6; P < .001). In the test set, the model yielded an AUC of 0.777 (95% CI, 0.775-0.779) for predicting risk of a creatinine level increase of at least 0.3 mg/dL, 0.839 (95% CI, 0.837-0.841) for predicting risk of a creatinine level increase of at least 0.5 mg/dL, and 0.870 (95% CI, 0.867-0.873) for predicting risk of a creatinine level increase of at least 1.0 mg/dL; it achieved a calibration slope of 0.998 (95% CI, 0.989-1.007), 0.999 (95% CI, 0.989-1.008), and 0.986 (95% CI, 0.973-0.998), respectively, for the AKI severity levels. The model had similar performance in the validation set (creatinine level increase of ≥0.3 mg/dL: AUC, 0.794; 95% CI, 0.792-0.795; calibration slope, 1.039; 95% CI, 1.030-1.047; creatinine level increase of ≥0.5 mg/dL: AUC, 0.845; 95% CI, 0.843-0.848; calibration slope, 1.063; 95% CI, 1.054-1.074; creatinine level increase of ≥1.0 mg/dL: AUC, 0.872; 95% CI, 0.869-0.875; calibration slope, 1.103; 95% CI, 1.089-1.117).
The association of contrast volume with AKI risk is complex, varies by baseline risk, and can be predicted by a model. Future research to evaluate the effect of the model on AKI is needed.
确定经皮冠状动脉介入治疗(PCI)过程中的对比剂用量与急性肾损伤(AKI)风险之间的关联对于优化 PCI 的安全性非常重要。
定量评估 AKI 风险与对比剂用量之间的关联,同时考虑到不同基线风险之间存在的非线性和异质性。
设计、设置和参与者:这是一项预后研究,使用了美国心脏病学会国家心血管数据注册中心的 CathPCI 登记处来自 1694 家美国医院的数据。推导分析包括 2076694 名于 2011 年 7 月 1 日至 2015 年 6 月 30 日期间接受 PCI 的患者。验证分析包括 961863 名于 2015 年 7 月 1 日至 2017 年 3 月 31 日期间接受 PCI 的患者。数据分析于 2018 年 7 月至 2019 年 5 月进行。
PCI 过程中的对比剂用量。
采用术前至术后肌酐水平升高(即≥0.3mg/dL、≥0.5mg/dL 和≥1.0mg/dL)的 3 个阈值来定义急性肾损伤。开发了一种用于定量评估对比剂用量与 AKI 之间关联的模型,并通过似然比检验来检查非线性和异质性的存在。该模型是在训练集中(从推导队列中随机抽取的 50%)开发的,并在测试集中(推导队列的其余 50%)和独立的验证集中评估了其性能,通过受试者工作特征曲线下面积(AUC)和观测与预测风险的校准斜率来评估。
推导集中的 2076694 例患者的平均(SD)年龄为 65.1(12.1)岁,其中 662525 例(31.9%)为女性;133306 例(6.4%)患者的肌酐水平升高至少 0.3mg/dL,66626 例(3.2%)患者的肌酐水平升高至少 0.5mg/dL,28378 例(1.4%)患者的肌酐水平升高至少 1.0mg/dL。在验证集中的 961843 例患者(平均[SD]年龄为 65.7[12.1]岁;305577 例[31.8%]为女性)中,这些比例分别为 62913(6.5%)、34229(3.6%)和 15555(1.6%)。对比剂用量与 AKI 风险之间的关联是非线性的(χ²26=1436.2;P<0.001),且因术前风险而异(χ²20=105.6;P<0.001)。在测试集中,该模型对预测肌酐水平升高≥0.3mg/dL 的风险的 AUC 为 0.777(95%CI,0.775-0.779),对预测肌酐水平升高≥0.5mg/dL 的风险的 AUC 为 0.839(95%CI,0.837-0.841),对预测肌酐水平升高≥1.0mg/dL 的风险的 AUC 为 0.870(95%CI,0.867-0.873);其校准斜率为 0.998(95%CI,0.989-1.007)、0.999(95%CI,0.989-1.008)和 0.986(95%CI,0.973-0.998),分别对应 AKI 严重程度等级。该模型在验证集中具有类似的性能(肌酐水平升高≥0.3mg/dL:AUC 为 0.794;95%CI,0.792-0.795;校准斜率为 1.039;95%CI,1.030-1.047;肌酐水平升高≥0.5mg/dL:AUC 为 0.845;95%CI,0.843-0.848;校准斜率为 1.063;95%CI,1.054-1.074;肌酐水平升高≥1.0mg/dL:AUC 为 0.872;95%CI,0.869-0.875;校准斜率为 1.103;95%CI,1.089-1.117)。
对比剂用量与 AKI 风险之间的关联是复杂的,因基线风险而异,可以通过模型进行预测。需要进一步研究该模型对 AKI 的影响。