Medical Research Council Clinical Trials Unit (MRC CTU) at UCL, Institute of Clinical Trials and Methodology, UCL, London, UK.
Department of Paediatrics, Mulago Hospital, Makerere University, Kampala, Uganda.
Crit Care. 2019 Nov 27;23(1):377. doi: 10.1186/s13054-019-2619-y.
African children hospitalised with severe febrile illness have a high risk of mortality. The Fluid Expansion As Supportive Therapy (FEAST) trial (ISCRTN 69856593) demonstrated increased mortality risk associated with fluid boluses, but the temporal relationship to bolus therapy and underlying mechanism remains unclear.
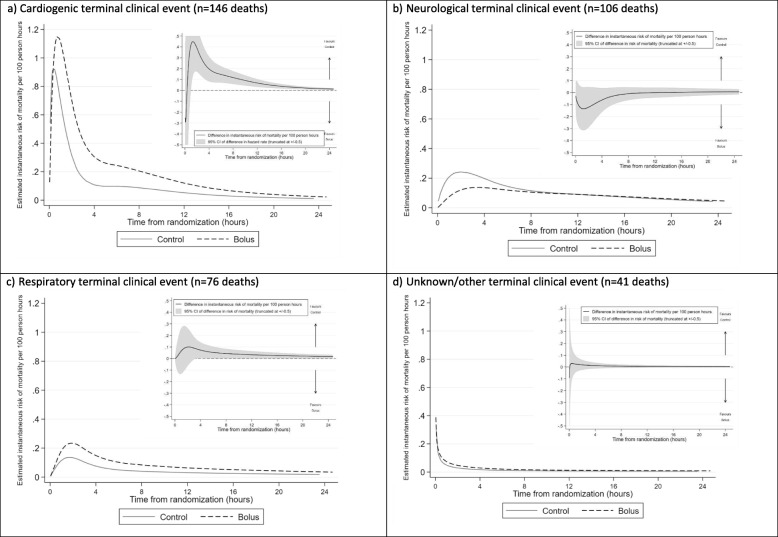
In a post hoc retrospective analysis, flexible parametric models were used to compare change in mortality risk post-randomisation in children allocated to bolus therapy with 20-40 ml/kg 5% albumin or 0.9% saline over 1-2 h or no bolus (control, 4 ml/kg/hour maintenance), overall and for different terminal clinical events (cardiogenic, neurological, respiratory, or unknown/other).
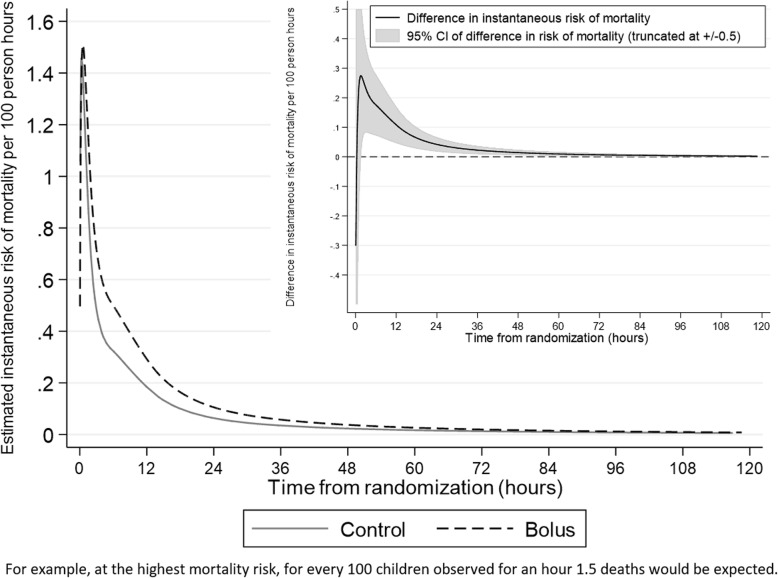
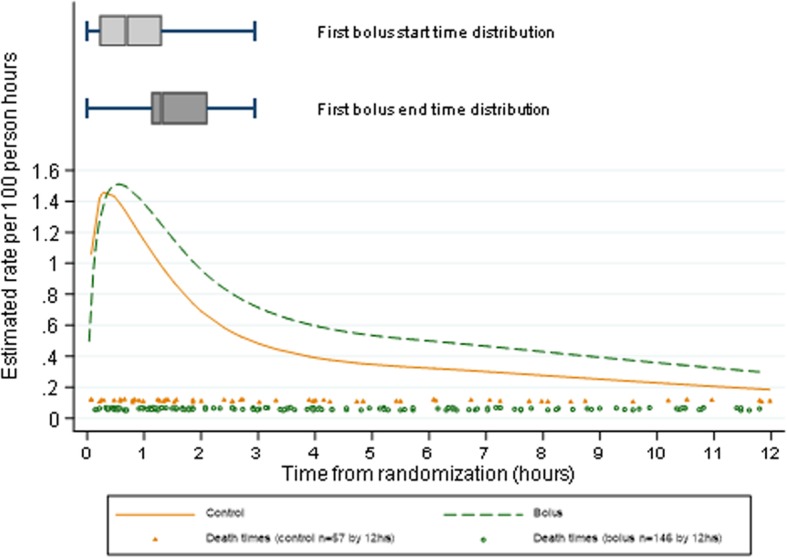
Two thousand ninety-seven and 1041 children were randomised to bolus vs no bolus, of whom 254 (12%) and 91 (9%) respectively died within 28 days. Median (IQR) bolus fluid in the bolus groups received by 4 h was 20 (20, 40) ml/kg and was the same at 8 h; total fluids received in bolus groups at 4 h and 8 h were 38 (28, 43) ml/kg and 40 (30, 50) ml/kg, respectively. Total fluid volumes received in the control group by 4 h and 8 h were median (IQR) 10 (6, 15) ml/kg and 10 (10, 26) ml/kg, respectively. Mortality risk was greatest 30 min post-randomisation in both groups, declining sharply to 4 h and then more slowly to 28 days. Maximum mortality risk was similar in bolus and no bolus groups; however, the risk declined more slowly in the bolus group, with significantly higher mortality risk compared to the no bolus group from 1.6 to 101 h (4 days) post-randomisation. The delay in decline in mortality risk in the bolus groups was most pronounced for cardiogenic modes of death.
The increased risk from bolus therapy was not due to a mechanism occurring immediately after bolus administration. Excess mortality risk in the bolus group resulted from slower decrease in mortality risk over the ensuing 4 days. Thus, administration of modest bolus volumes appeared to prevent mortality risk declining at the same rate that it would have done without a bolus, rather than harm associated with bolus resulting from a concurrent increased risk of death peri-bolus administration.
ISRCTN69856593. Date of registration 15 December 2008.
在因严重发热性疾病住院的非洲儿童中,死亡率较高。液体扩张作为支持性治疗(FEAST)试验(ISCRTN 69856593)表明,与液体冲击疗法相关的死亡率风险增加,但冲击疗法与潜在机制之间的时间关系尚不清楚。
在一项事后回顾性分析中,采用灵活的参数模型比较了随机分组后不同治疗组儿童在 28 天内的死亡率风险变化。分组为冲击治疗组(20-40ml/kg 5%白蛋白或 0.9%生理盐水,1-2 小时内输入)和对照组(4ml/kg/h 维持治疗)。
2097 名和 1041 名儿童分别被随机分配到冲击治疗组和对照组,其中 254 名(12%)和 91 名(9%)儿童分别在 28 天内死亡。冲击治疗组在 4 小时时中位数(IQR)接受的冲击液量为 20(20,40)ml/kg,8 小时时相同;冲击治疗组在 4 小时和 8 小时时接受的总液体量分别为 38(28,43)ml/kg 和 40(30,50)ml/kg。对照组在 4 小时和 8 小时时接受的总液体量中位数(IQR)分别为 10(6,15)ml/kg 和 10(10,26)ml/kg。死亡率风险在两组中均在随机分组后 30 分钟达到最高,然后在 4 小时急剧下降,然后缓慢下降至 28 天。冲击治疗组和对照组的最大死亡率风险相似;然而,在冲击治疗组,死亡率风险下降较慢,与对照组相比,从随机分组后 1.6 至 101 小时(4 天)时的死亡率风险明显更高。在冲击治疗组中,心源性死亡模式的死亡率风险下降延迟最为明显。
冲击治疗带来的风险增加并不是由于冲击治疗后立即发生的机制引起的。冲击治疗组的超额死亡率风险是由于在随后的 4 天内死亡率风险下降速度较慢所致。因此,给予适量的冲击液量似乎可以防止死亡率风险以与没有冲击治疗相同的速度下降,而不是与冲击治疗相关的危害,即冲击治疗后 4 小时内死亡率风险增加。
ISRCTN69856593。注册日期:2008 年 12 月 15 日。