Department of Cardiology, Herlev and Gentofte Hospital, University of Copenhagen, Copenhagen, Denmark.
Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
ESC Heart Fail. 2020 Feb;7(1):147-157. doi: 10.1002/ehf2.12532. Epub 2019 Dec 9.
We hypothesized that grading of diastolic dysfunction (DDF) according to two DDF grading algorithms and strain imaging yields prognostic information on all-cause mortality in patients with heart failure with reduced ejection fraction (HFrEF).
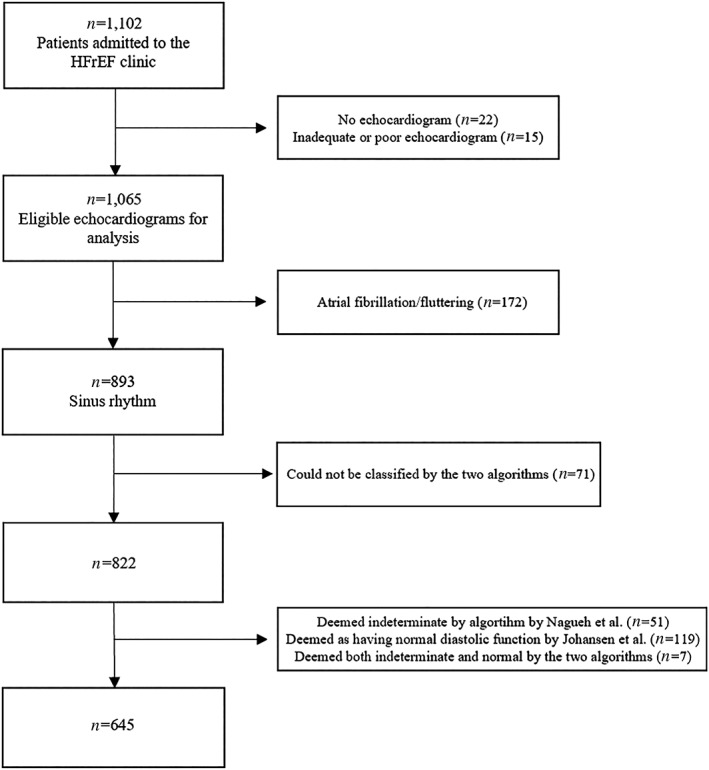
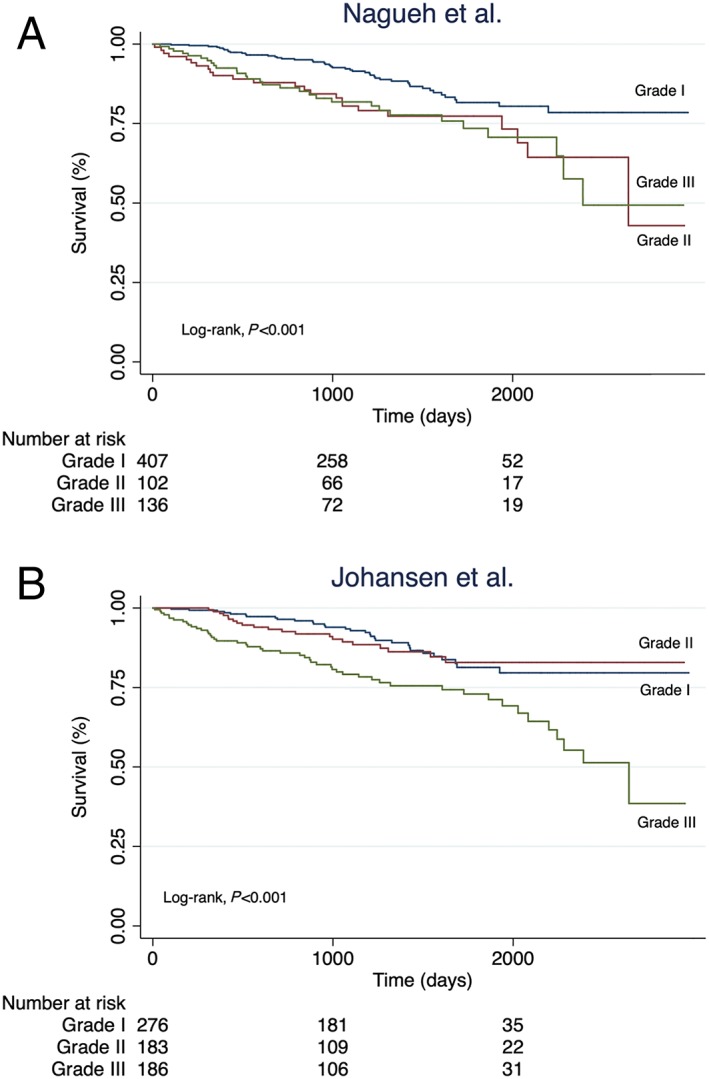
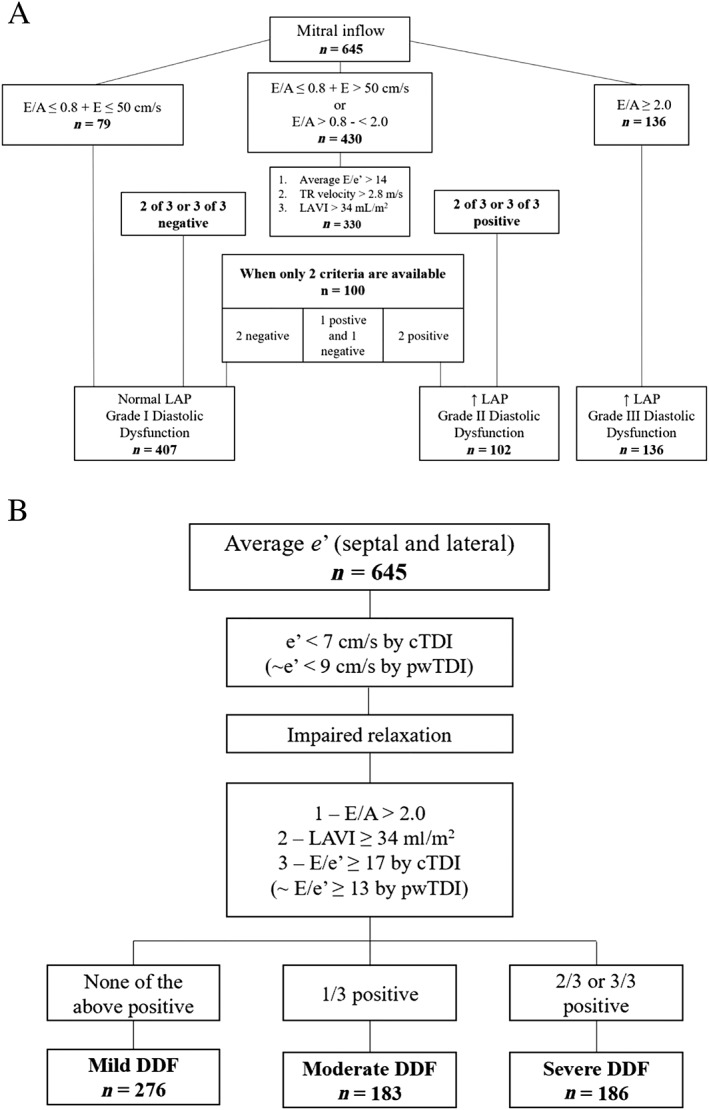
We enrolled ambulatory HFrEF (left ventricular ejection fraction < 45%; N = 1 065) patients who underwent echocardiography and speckle tracking assessment of global longitudinal strain (GLS). Patients were stratified according to DDF grades (Grades I-III) according to two contemporary DDF grading algorithms. Prognostic performance was assessed by C-statistics. Of the originally 1 065 enrolled patients, a total of 645 (61%) patients (age: 67 ± 11 years, male: 72%, ejection fraction: 27 ± 9%) were classified according to both DDF grading algorithms. Concordance between the algorithms was moderate (kappa = 0.48) and the reclassification rate was 33%. During a median follow-up of 3.3 years (1.9, 4.7 years), 101 (16%) died from all causes. When comparing DDF Grade I vs. Grade III, both algorithms provided prognostic information [Nagueh: (hazard ratio) HR 2.09, 95% confidence interval (CI),1.32-3.31, P = 0.002; Johansen: HR 2.47, 95% CI, 1.57-3.87, P < 0.001]. However, when comparing DDF Grade II vs. Grade III, only the Johansen algorithm yielded prognostic information (Nagueh: HR 1.04, 95% CI, 0.60-1.77, P = 0.90; Johansen: HR 2.26, 95% CI, 1.35-3.77, P = 0.002). We found no difference in prognostic performance between the two algorithms (C-statistics: 0.604 vs. 0.623, P = 0.24). Assessed by C-statistics, the most powerful predictors of the endpoint from the two algorithms were E/e'-ratio (C-statistics: 0.644), tricuspid regurgitation velocity (C-statistics: 0.625) and E/A-ratio (C-statistics: 0.602). When adding GLS to a combination of these predictors, the prognostic performance increased significantly (C-statistics: 0.705 vs. C-statistics: 0.634, P = 0.028).
Evaluation of DDF in patients with HFrEF yields prognostic information on all-cause mortality. Furthermore, adding GLS to contemporary algorithms of DDF adds novel prognostic information.
我们假设根据两种舒张功能不全(DDF)分级算法和应变成像对舒张功能不全进行分级,可以为射血分数降低的心力衰竭(HFrEF)患者的全因死亡率提供预后信息。
我们招募了接受超声心动图和斑点追踪评估整体纵向应变(GLS)的有症状的 HFrEF(左心室射血分数<45%;N=1065)患者。根据两种当代 DDF 分级算法,患者根据 DDF 分级(I-III 级)进行分层。通过 C 统计量评估预后性能。在最初纳入的 1065 名患者中,共有 645 名(61%)患者(年龄:67±11 岁,男性:72%,射血分数:27±9%)根据两种 DDF 分级算法进行了分类。两种算法之间的一致性为中度(kappa=0.48),重新分类率为 33%。在中位随访 3.3 年(1.9,4.7 年)期间,有 101 名(16%)患者因各种原因死亡。与 DDF 分级 I 相比,DDF 分级 III,两种算法均提供预后信息[纳盖:(危险比)HR 2.09,95%置信区间(CI),1.32-3.31,P=0.002;约翰森:HR 2.47,95%CI,1.57-3.87,P<0.001]。然而,与 DDF 分级 II 相比,仅约翰森算法提供了预后信息(纳盖:HR 1.04,95%CI,0.60-1.77,P=0.90;约翰森:HR 2.26,95%CI,1.35-3.77,P=0.002)。我们没有发现两种算法之间预后性能的差异(C 统计量:0.604 与 0.623,P=0.24)。通过 C 统计量评估,两种算法中预测终点的最有力指标是 E/e'-比值(C 统计量:0.644)、三尖瓣反流速度(C 统计量:0.625)和 E/A 比值(C 统计量:0.602)。当将 GLS 添加到这些预测指标的组合中时,预后性能显著提高(C 统计量:0.705 与 C 统计量:0.634,P=0.028)。
评估 HFrEF 患者的 DDF 可提供全因死亡率的预后信息。此外,将 GLS 添加到 DDF 的当代算法中可提供新的预后信息。