Department of Medical Microbiology and Immunology, Rijnstate Hospital, Wagnerlaan 55, 6815 AD, Arnhem, the Netherlands.
Department of Mathematics, University Utrecht, Utrecht, the Netherlands.
Crit Care. 2019 Dec 12;23(1):408. doi: 10.1186/s13054-019-2687-z.
To develop a mathematical model to estimate daily evolution of disease severity using routinely available parameters in patients admitted to the intensive care unit (ICU).
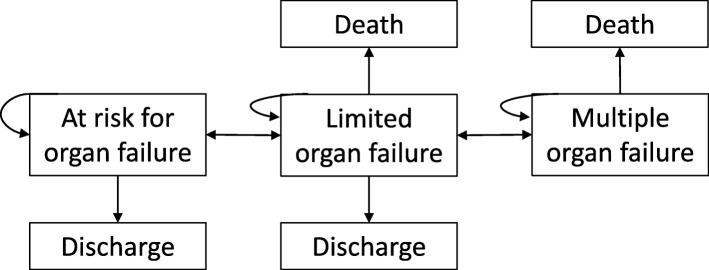
Over a 3-year period, we prospectively enrolled consecutive adults with sepsis and categorized patients as (1) being at risk for developing (more severe) organ dysfunction, (2) having (potentially still reversible) limited organ failure, or (3) having multiple-organ failure. Daily probabilities for transitions between these disease states, and to death or discharge, during the first 2 weeks in ICU were calculated using a multi-state model that was updated every 2 days using both baseline and time-varying information. The model was validated in independent patients.
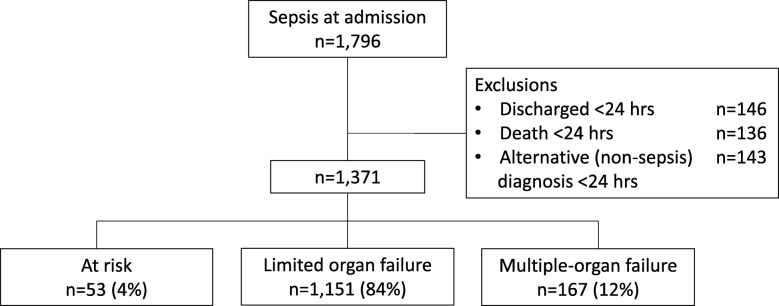
We studied 1371 sepsis admissions in 1251 patients. Upon presentation, 53 (4%) were classed at risk, 1151 (84%) had limited organ failure, and 167 (12%) had multiple-organ failure. Among patients with limited organ failure, 197 (17%) evolved to multiple-organ failure or died and 809 (70%) improved or were discharged alive within 14 days. Among patients with multiple-organ failure, 67 (40%) died and 91 (54%) improved or were discharged. Treatment response could be predicted with reasonable accuracy (c-statistic ranging from 0.55 to 0.81 for individual disease states, and 0.67 overall). Model performance in the validation cohort was similar.
This prediction model that estimates daily evolution of disease severity during sepsis may eventually support clinicians in making better informed treatment decisions and could be used to evaluate prognostic biomarkers or perform in silico modeling of novel sepsis therapies during trial design.
ClinicalTrials.gov NCT01905033.
开发一种数学模型,使用重症监护病房(ICU)中常规可用的参数来估计疾病严重程度的每日变化。
在 3 年期间,我们前瞻性地连续招募患有败血症的成年患者,并将患者分为(1)有发展(更严重)器官功能障碍风险的患者,(2)有(潜在的仍然可逆)有限器官衰竭的患者,或(3)有多器官衰竭的患者。使用多状态模型计算这些疾病状态之间以及 ICU 前 2 周内死亡或出院的每日转移概率,该模型每 2 天使用基线和时变信息进行更新。该模型在独立患者中进行了验证。
我们研究了 1251 名患者中的 1371 例败血症入院。就诊时,53 例(4%)被归类为有风险,1151 例(84%)有有限的器官衰竭,167 例(12%)有多个器官衰竭。在有限器官衰竭的患者中,197 例(17%)发展为多器官衰竭或死亡,809 例(70%)在 14 天内好转或出院。在多器官衰竭的患者中,67 例(40%)死亡,91 例(54%)好转或出院。治疗反应可以合理准确地预测(个体疾病状态的 C 统计量范围为 0.55 至 0.81,总体为 0.67)。验证队列中的模型性能相似。
该预测模型可估计败血症期间疾病严重程度的每日变化,最终可能有助于临床医生做出更明智的治疗决策,并可用于评估预后生物标志物或在试验设计中进行新型败血症治疗的计算机模拟。
ClinicalTrials.gov NCT01905033。