Centre for Clinical Research Sörmland, Uppsala University, Eskilstuna, Sweden.
Department of Community Medicine and Rehabilitation, Physiotherapy, Umeå University, Umeå, Sweden.
BMJ Open. 2019 Dec 11;9(12):e032560. doi: 10.1136/bmjopen-2019-032560.
Weaknesses of the nine-hole peg test include high floor effects and a result that might be difficult to interpret. In the twenty-five-hole peg test (TFHPT), the larger number of available pegs allows for the straightforward counting of the number of pegs inserted as the result. The TFHPT provides a comprehensible result and low floor effects. The objective was to assess the test-retest reliability of the TFHPT when testing persons with stroke. A particular focus was placed on the absolute reliability, as quantified by the smallest real difference (SRD). Complementary aims were to investigate possible implications for how the TFHPT should be used and for how the SRD of the TFHPT performance should be expressed.
This study employed a test-retest design including three trials. The pause between trials was approximately 10-120 s.
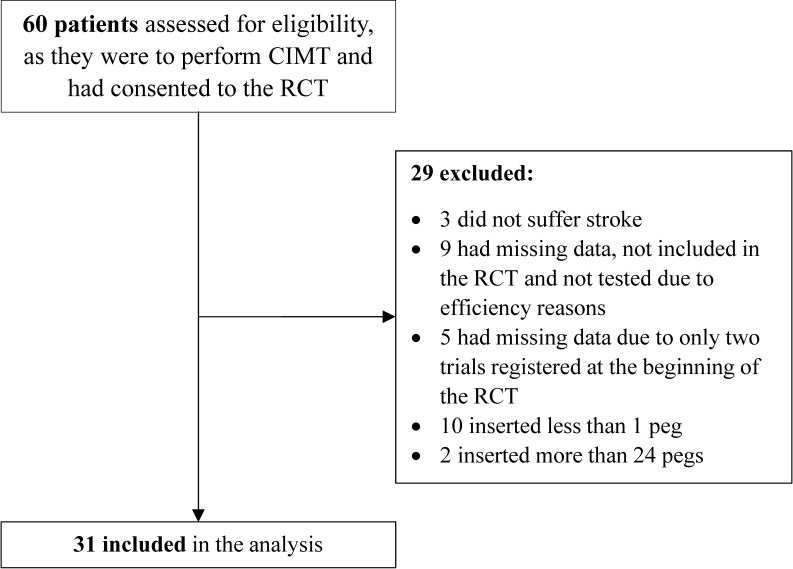
PARTICIPANTS, SETTING AND OUTCOME MEASURE: Thirty-one participants who had suffered a stroke were recruited from a group designated for constraint-induced movement therapy at outpatient clinics. The TFHPT result was expressed as the number of pegs inserted.
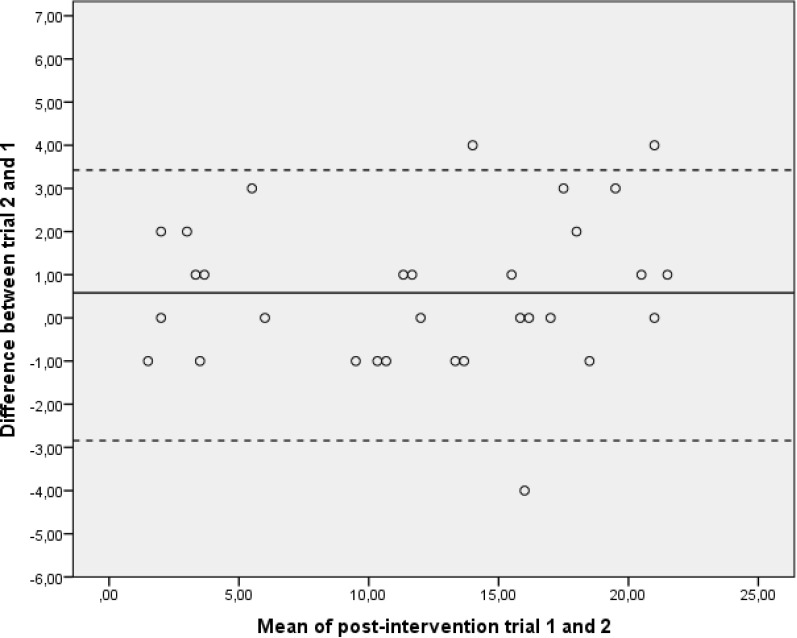
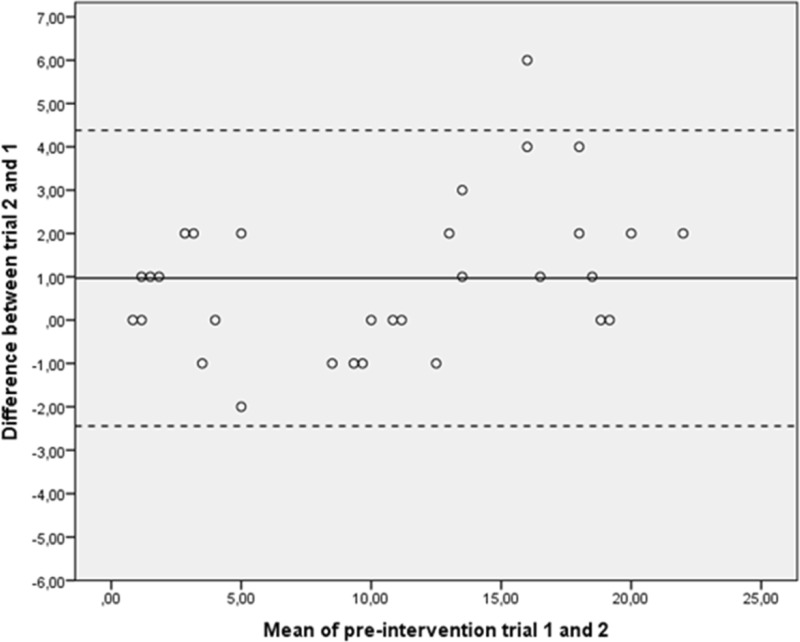
Absolute reliability was quantified by the SRD, including random and systematic error for a single trial, SRD, and for an average of three trials, SRD. For the SRD measures, the corresponding SRD percentage (SRD%) measure was also reported.
The differences in the number of pegs necessary to detect a change in the TFHPT for SRD and SRD were 4.0 and 2.3, respectively. The corresponding SRD% values for SRD and SRD were 36.5% and 21.3%, respectively.
The smallest change that can be detected in the TFHPT should be just above two pegs for a test procedure including an average of three trials. The use of an average of three trials compared with a single trial substantially reduces the measurement error.
ISRCTN registry, reference number ISRCTN24868616.
九孔钉测试的弱点包括高地板效应和结果难以解释。在二十五孔钉测试(TFHPT)中,可用钉的数量较多,可以直接计数插入的钉数作为结果。TFHPT 提供了一个易于理解的结果和低地板效应。目的是评估 TFHPT 在测试中风患者时的测试-重测信度。特别关注绝对信度,用最小真实差异(SRD)来量化。补充目标是研究如何使用 TFHPT 和如何表达 TFHPT 性能的 SRD。
本研究采用了测试-重测设计,包括三次试验。两次试验之间的停顿时间约为 10-120 秒。
参与者、设置和结果测量:从门诊诊所指定的强制性运动疗法组中招募了 31 名中风患者。TFHPT 结果表示为插入的钉数。
绝对信度通过 SRD 量化,包括单次试验的随机和系统误差、SRD 和三次试验的平均 SRD。对于 SRD 测量,还报告了相应的 SRD%测量值。
为了检测 TFHPT 中的变化,SRD 和 SRD 所需的钉数差异分别为 4.0 和 2.3。相应的 SRD%值分别为 36.5%和 21.3%。
在包括三次试验的平均测试程序中,TFHPT 中可以检测到的最小变化应该刚好超过两个钉。与单次试验相比,使用三次试验的平均值可以大大降低测量误差。
ISRCTN 注册表,参考号 ISRCTN24868616。