Division of Gastroenterology, The Second Affiliated Hospital, Xi'an Jiaotong University, Xi'an 710004, Shaanxi Province, China.
World J Gastroenterol. 2019 Dec 7;25(45):6668-6680. doi: 10.3748/wjg.v25.i45.6668.
Acute variceal bleeding is one of the deadliest complications of cirrhosis, with a high risk of in-hospital rebleeding and mortality. Some risk scoring systems to predict clinical outcomes in patients with upper gastrointestinal bleeding have been developed. However, for cirrhotic patients with variceal bleeding, data regarding the predictive value of these prognostic scores in predicting in-hospital outcomes are limited and controversial.
To validate and compare the overall performance of selected prognostic scoring systems for predicting in-hospital outcomes in cirrhotic patients with variceal bleeding.
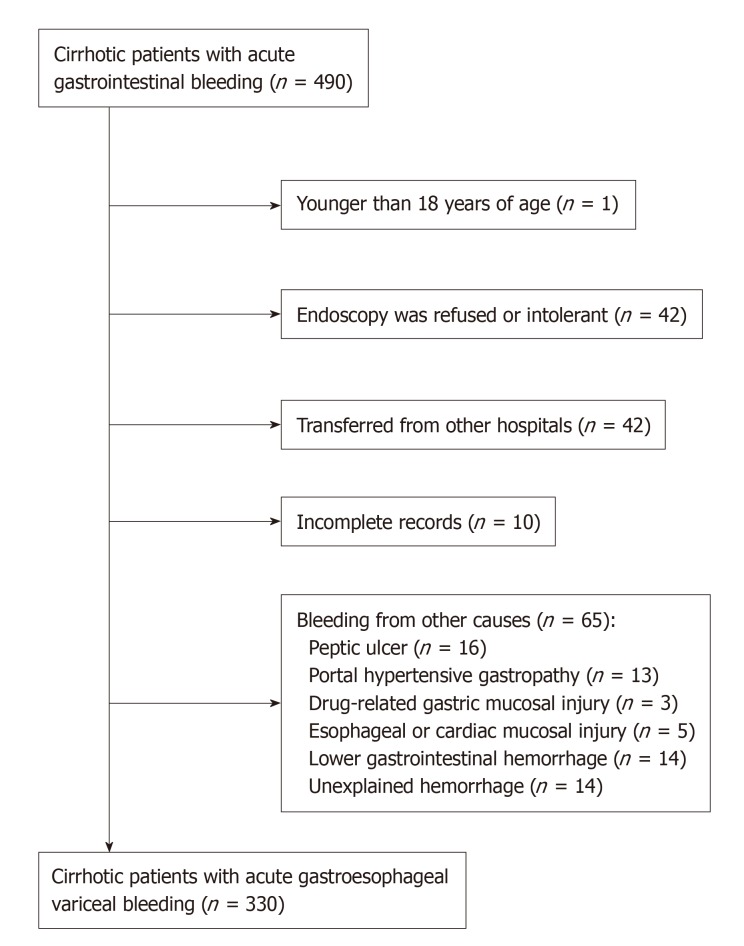
From March 2017 to June 2019, cirrhotic patients with acute variceal bleeding were retrospectively enrolled at the Second Affiliated Hospital of Xi'an Jiaotong University. The clinical Rockall score (CRS), AIMS65 score (AIMS65), Glasgow-Blatchford score (GBS), modified GBS (mGBS), Canada-United Kingdom-Australia score (CANUKA), Child-Turcotte-Pugh score (CTP), model for end-stage liver disease (MELD) and MELD-Na were calculated. The overall performance of these prognostic scoring systems was evaluated.
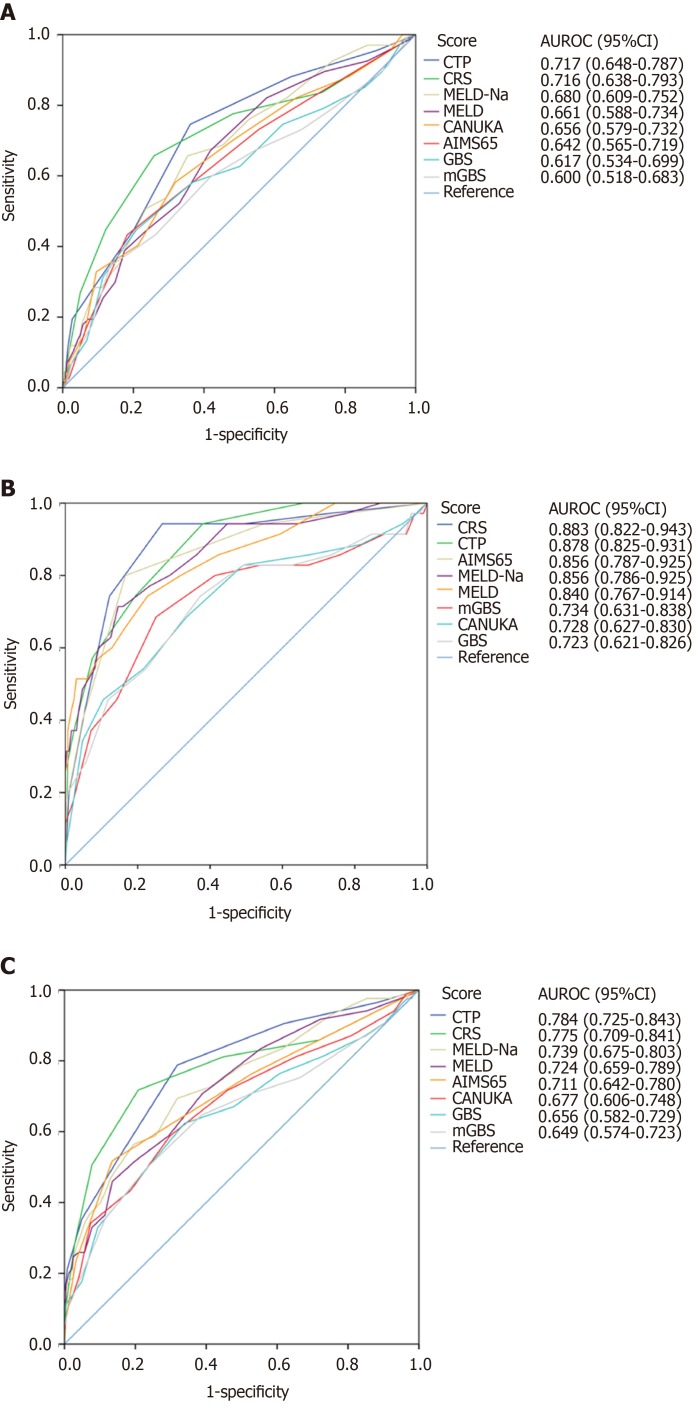
A total of 330 cirrhotic patients with variceal bleeding were enrolled; the rates of in-hospital rebleeding and mortality were 20.3% and 10.6%, respectively. For in-hospital rebleeding, the discriminative ability of the CTP and CRS were clinically acceptable, with area under the receiver operating characteristic curves (AUROCs) of 0.717 (0.648-0.787) and 0.716 (0.638-0.793), respectively. The other tested scoring systems had poor discriminative ability (AUROCs < 0.7). For in-hospital mortality, the CRS, CTP, AIMS65, MELD-Na and MELD showed excellent discriminative ability (AUROCs > 0.8). The AUROCs of the mGBS, CANUKA and GBS were relatively small, but clinically acceptable (AUROCs > 0.7). Furthermore, the calibration of all scoring systems was good for either in-hospital rebleeding or death.
For cirrhotic patients with variceal bleeding, in-hospital rebleeding and mortality rates remain high. The CTP and CRS can be used clinically to predict in-hospital rebleeding. The performances of the CRS, CTP, AIMS65, MELD-Na and MELD are excellent at predicting in-hospital mortality.
急性静脉曲张出血是肝硬化最致命的并发症之一,具有院内再出血和死亡率高的风险。已经开发了一些用于预测上消化道出血患者临床结局的风险评分系统。然而,对于肝硬化静脉曲张出血患者,关于这些预后评分预测院内结局的预测价值的数据有限且存在争议。
验证和比较选定的预后评分系统在预测肝硬化静脉曲张出血患者院内结局方面的总体表现。
2017 年 3 月至 2019 年 6 月,西安交通大学第二附属医院回顾性纳入肝硬化急性静脉曲张出血患者。计算临床 Rockall 评分(CRS)、AIMS65 评分(AIMS65)、格拉斯哥-布拉奇福德评分(GBS)、改良 GBS(mGBS)、加拿大-英国-澳大利亚评分(CANUKA)、Child-Turcotte-Pugh 评分(CTP)、终末期肝病模型(MELD)和 MELD-Na。评估这些预后评分系统的总体表现。
共纳入 330 例肝硬化静脉曲张出血患者,院内再出血和死亡率分别为 20.3%和 10.6%。对于院内再出血,CTP 和 CRS 的判别能力具有临床可接受性,其受试者工作特征曲线下面积(AUROCs)分别为 0.717(0.648-0.787)和 0.716(0.638-0.793)。其他测试的评分系统具有较差的判别能力(AUROCs<0.7)。对于院内死亡率,CRS、CTP、AIMS65、MELD-Na 和 MELD 显示出优异的判别能力(AUROCs>0.8)。mGBS、CANUKA 和 GBS 的 AUROCs 相对较小,但具有临床可接受性(AUROCs>0.7)。此外,所有评分系统对于院内再出血或死亡的校准均良好。
对于肝硬化静脉曲张出血患者,院内再出血和死亡率仍然很高。CTP 和 CRS 可用于临床预测院内再出血。CRS、CTP、AIMS65、MELD-Na 和 MELD 在预测院内死亡率方面表现出色。