Stanley Adrian J, Laine Loren, Dalton Harry R, Ngu Jing H, Schultz Michael, Abazi Roseta, Zakko Liam, Thornton Susan, Wilkinson Kelly, Khor Cristopher J L, Murray Iain A, Laursen Stig B
Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK
Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, CT, USA.
BMJ. 2017 Jan 4;356:i6432. doi: 10.1136/bmj.i6432.
To compare the predictive accuracy and clinical utility of five risk scoring systems in the assessment of patients with upper gastrointestinal bleeding.
International multicentre prospective study.
Six large hospitals in Europe, North America, Asia, and Oceania.
3012 consecutive patients presenting over 12 months with upper gastrointestinal bleeding.
Comparison of pre-endoscopy scores (admission Rockall, AIMS65, and Glasgow Blatchford) and post-endoscopy scores (full Rockall and PNED) for their ability to predict predefined clinical endpoints: a composite endpoint (transfusion, endoscopic treatment, interventional radiology, surgery, or 30 day mortality), endoscopic treatment, 30 day mortality, rebleeding, and length of hospital stay. Optimum score thresholds to identify low risk and high risk patients were determined.
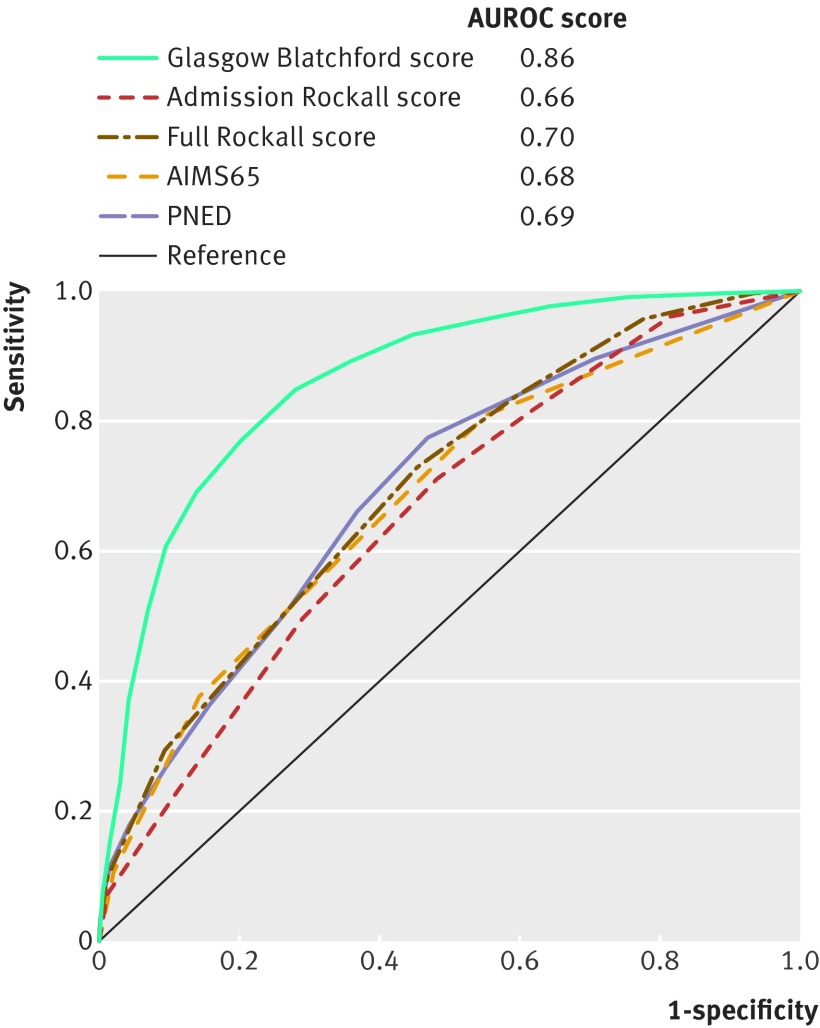
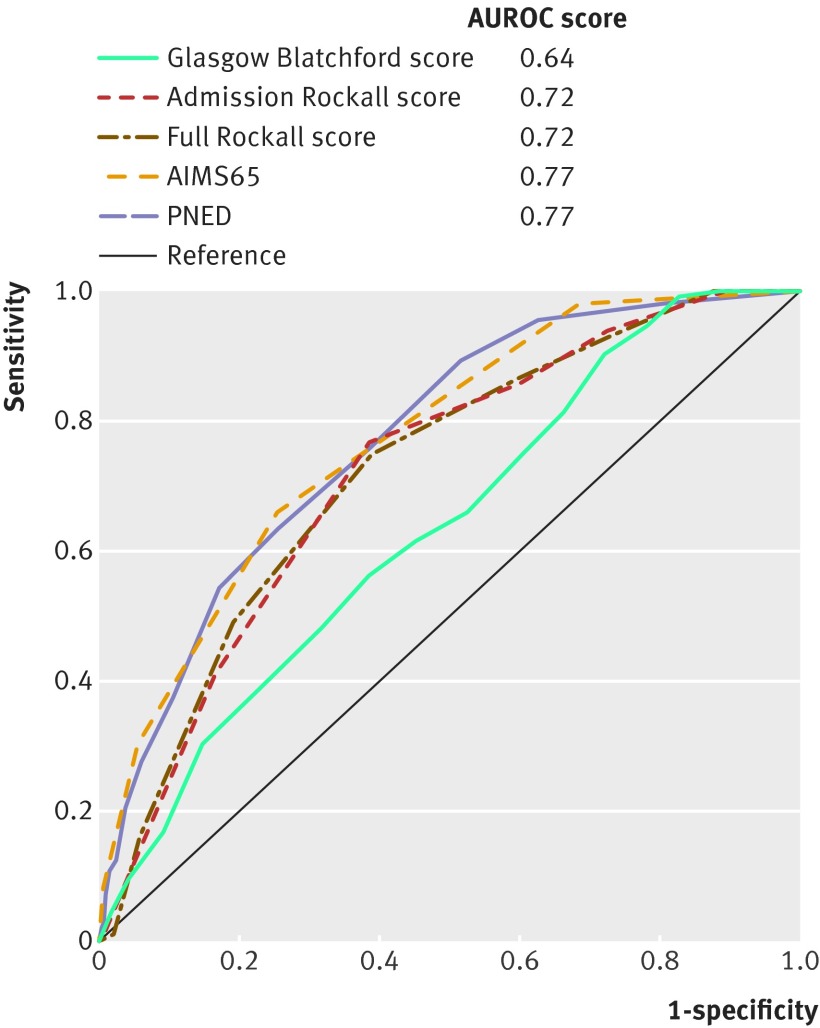
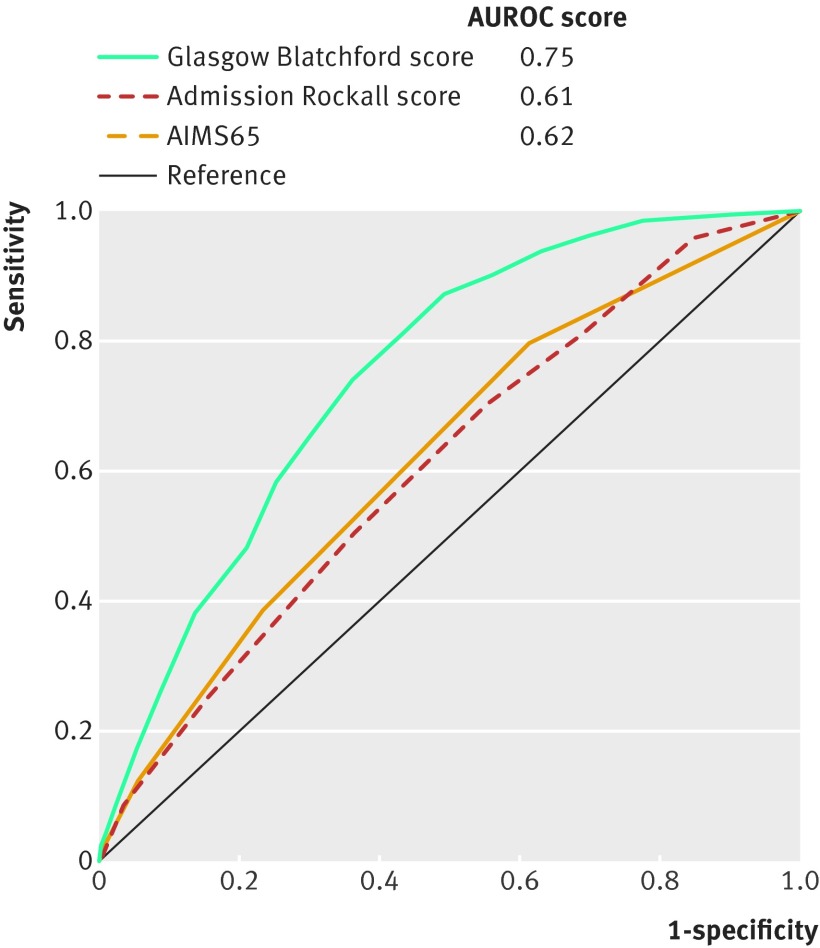
The Glasgow Blatchford score was best (area under the receiver operating characteristic curve (AUROC) 0.86) at predicting intervention or death compared with the full Rockall score (0.70), PNED score (0.69), admission Rockall score (0.66, and AIMS65 score (0.68) (all P<0.001). A Glasgow Blatchford score of ≤1 was the optimum threshold to predict survival without intervention (sensitivity 98.6%, specificity 34.6%). The Glasgow Blatchford score was better at predicting endoscopic treatment (AUROC 0.75) than the AIMS65 (0.62) and admission Rockall scores (0.61) (both P<0.001). A Glasgow Blatchford score of ≥7 was the optimum threshold to predict endoscopic treatment (sensitivity 80%, specificity 57%). The PNED (AUROC 0.77) and AIMS65 scores (0.77) were best at predicting mortality, with both superior to admission Rockall score (0.72) and Glasgow Blatchford score (0.64; P<0.001). Score thresholds of ≥4 for PNED, ≥2 for AIMS65, ≥4 for admission Rockall, and ≥5 for full Rockall were optimal at predicting death, with sensitivities of 65.8-78.6% and specificities of 65.0-65.3%. No score was helpful at predicting rebleeding or length of stay.
The Glasgow Blatchford score has high accuracy at predicting need for hospital based intervention or death. Scores of ≤1 appear the optimum threshold for directing patients to outpatient management. AUROCs of scores for the other endpoints are less than 0.80, therefore their clinical utility for these outcomes seems to be limited.Trial registration Current Controlled Trials ISRCTN16235737.
比较五种风险评分系统在上消化道出血患者评估中的预测准确性和临床实用性。
国际多中心前瞻性研究。
欧洲、北美、亚洲和大洋洲的六家大型医院。
连续12个月以上出现上消化道出血的3012例患者。
比较内镜检查前评分(入院时的罗卡尔评分、AIMS65评分和格拉斯哥布拉奇福德评分)和内镜检查后评分(完整罗卡尔评分和PNED评分)预测预定义临床终点的能力:复合终点(输血、内镜治疗、介入放射学、手术或30天死亡率)、内镜治疗、30天死亡率、再出血和住院时间。确定识别低风险和高风险患者的最佳评分阈值。
与完整罗卡尔评分(0.70)、PNED评分(0.69)、入院时罗卡尔评分(0.66)和AIMS65评分(0.68)相比,格拉斯哥布拉奇福德评分在预测干预或死亡方面表现最佳(受试者操作特征曲线下面积(AUROC)为0.86)(所有P<0.001)。格拉斯哥布拉奇福德评分≤1是预测无需干预即可存活的最佳阈值(敏感性98.6%,特异性34.6%)。格拉斯哥布拉奇福德评分在预测内镜治疗方面(AUROC为0.75)优于AIMS65评分(0.62)和入院时罗卡尔评分(0.61)(均P<0.001)。格拉斯哥布拉奇福德评分≥7是预测内镜治疗的最佳阈值(敏感性80%,特异性57%)。PNED评分(AUROC为0.77)和AIMS65评分(0.77)在预测死亡率方面表现最佳,均优于入院时罗卡尔评分(0.72)和格拉斯哥布拉奇福德评分(0.64;P<0.001)。PNED评分≥4、AIMS65评分≥2、入院时罗卡尔评分≥4和完整罗卡尔评分≥5是预测死亡的最佳阈值,敏感性为65.8 - 78.6%,特异性为65.0 - 65.3%。没有评分对预测再出血或住院时间有帮助。
格拉斯哥布拉奇福德评分在预测基于医院的干预需求或死亡方面具有较高准确性。评分≤1似乎是指导患者进行门诊管理的最佳阈值。其他终点评分的AUROC小于0.80,因此它们对这些结局的临床实用性似乎有限。试验注册号:当前受控试验ISRCTN16235737。