Lang Irene M, Palazzini Massimiliano
Department of Internal Medicine II, Medical University of Vienna, Währinger Gürtel 18-20, 1090 Vienna, Austria.
Department of Experimental, Diagnostic and Specialty Medicine, University of Bologna, Via Zamboni, 33 - 40126 Bologna, Italy.
Eur Heart J Suppl. 2019 Dec;21(Suppl K):K21-K28. doi: 10.1093/eurheartj/suz205. Epub 2019 Dec 17.
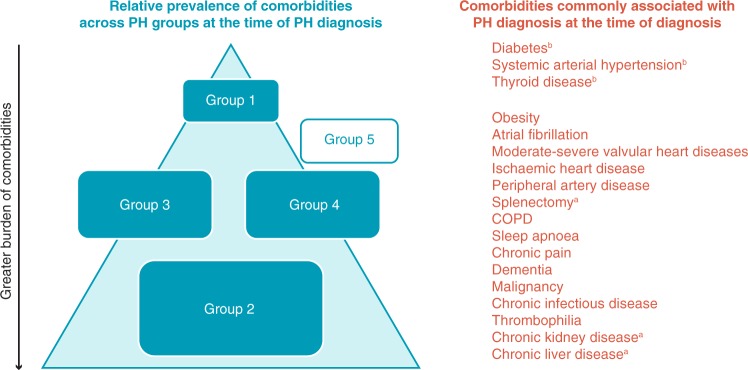
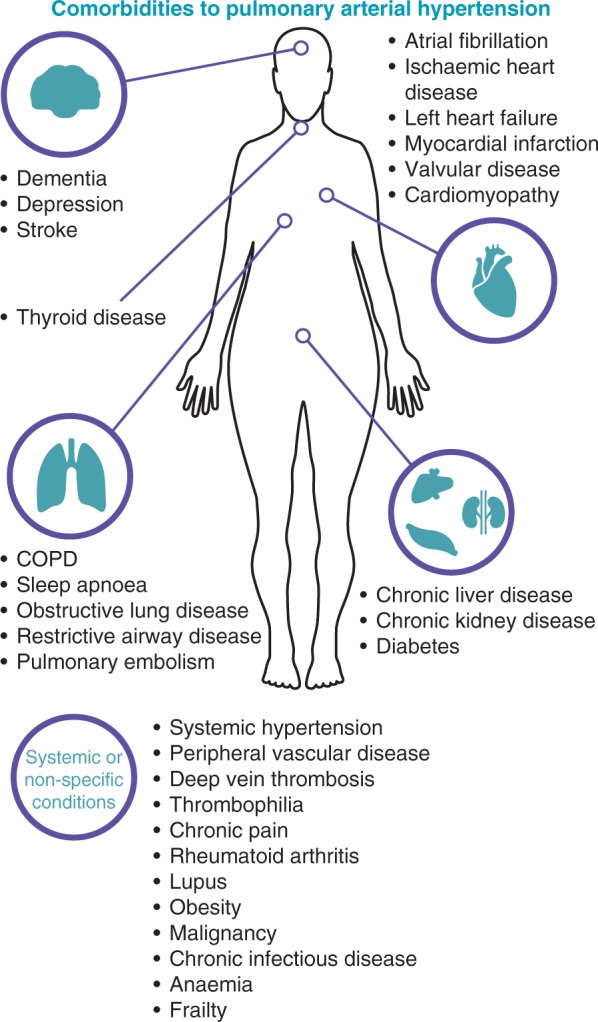
Patients with comorbidities are often excluded from clinical trials, limiting the evidence base for pulmonary arterial hypertension (PAH)-specific therapies. This review aims to discuss the effect of comorbidities on the diagnosis and management of PAH. The comorbidities discussed in this review (systemic hypertension, obesity, sleep apnoea, clinical depression, obstructive airway disease, thyroid disease, diabetes, and ischaemic cardiovascular event) were chosen based on their prevalence in patients with idiopathic PAH in the REVEAL registry (Registry to EValuate Early and Long-term PAH disease management). Comorbidities can mask the symptoms of PAH, leading to delays in diagnosis and also difficulty evaluating disease progression and treatment effects. Due to the multifactorial pathophysiology of pulmonary hypertension (PH), the presence of comorbidities can lead to difficulties in distinguishing between Group 1 PH (PAH) and the other group classifications of PH. Many comorbidities contribute to the progression of PAH through increased pulmonary artery pressures and cardiac output, therefore treatment of the comorbidity may also reduce the severity of PAH. Similarly, the development of one comorbidity can be a risk factor for the development of other comorbidities. The management of comorbidities requires consideration of drug interactions, polypharmacy, adherence and evidence-based strategies. A multidisciplinary team should be involved in the management of patients with PAH and comorbidities, with appropriate referral to supportive services when necessary. The treatment goals and expectations of patients must be managed in the context of comorbidities.
患有合并症的患者通常被排除在临床试验之外,这限制了肺动脉高压(PAH)特异性疗法的证据基础。本综述旨在讨论合并症对PAH诊断和管理的影响。本综述中讨论的合并症(系统性高血压、肥胖、睡眠呼吸暂停、临床抑郁症、阻塞性气道疾病、甲状腺疾病、糖尿病和缺血性心血管事件)是根据它们在REVEAL注册研究(评估PAH疾病早期和长期管理的注册研究)中特发性PAH患者中的患病率选择的。合并症可能会掩盖PAH的症状,导致诊断延迟,也难以评估疾病进展和治疗效果。由于肺动脉高压(PH)的多因素病理生理学,合并症的存在可能导致难以区分1组PH(PAH)和其他组别的PH分类。许多合并症通过增加肺动脉压力和心输出量促进PAH的进展,因此治疗合并症也可能降低PAH的严重程度。同样,一种合并症的发生可能是其他合并症发生的危险因素。合并症的管理需要考虑药物相互作用、多种药物治疗、依从性和循证策略。一个多学科团队应参与PAH合并合并症患者的管理,必要时适当转诊至支持性服务机构。必须在合并症的背景下管理患者的治疗目标和期望。