Division of Pulmonary and Critical Care, Intermountain Medical Center, Shock Trauma ICU, 5121 S. Cottonwood Street, Murray, UT, 84107, USA.
Division of Pulmonary and Critical Care, University of Utah, Salt Lake City, UT, USA.
Crit Care. 2019 Dec 27;23(1):424. doi: 10.1186/s13054-019-2698-9.
In patients with acute respiratory distress syndrome (ARDS), low tidal volume ventilation has been associated with reduced mortality. Driving pressure (tidal volume normalized to respiratory system compliance) may be an even stronger predictor of ARDS survival than tidal volume. We sought to study whether these associations hold true in acute respiratory failure patients without ARDS.
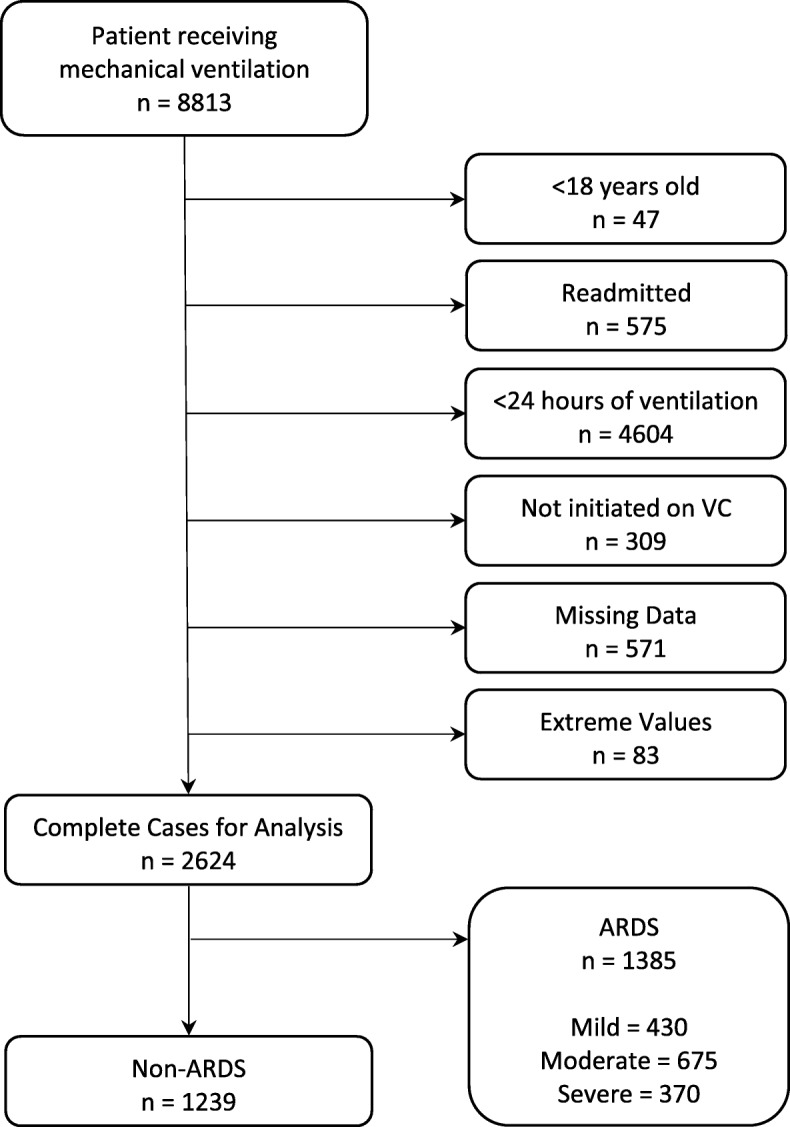
This is a retrospectively cohort analysis of mechanically ventilated adult patients admitted to ICUs from 12 hospitals over 2 years. We used natural language processing of chest radiograph reports and data from the electronic medical record to identify patients who had ARDS. We used multivariable logistic regression and generalized linear models to estimate associations between tidal volume, driving pressure, and respiratory system compliance with adjusted 30-day mortality using covariates of Acute Physiology Score (APS), Charlson Comorbidity Index (CCI), age, and PaO/FiO ratio.
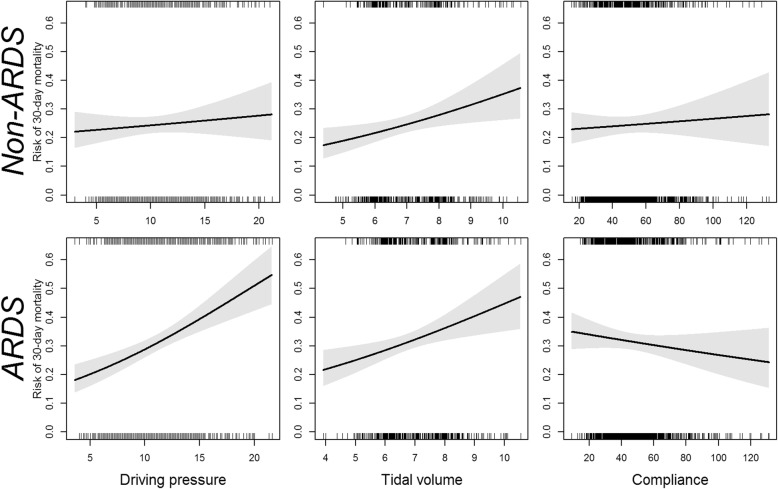
We studied 2641 patients; 48% had ARDS (n = 1273). Patients with ARDS had higher mean APS (25 vs. 23, p < .001) but similar CCI (4 vs. 3, p = 0.6) scores. For non-ARDS patients, tidal volume was associated with increased adjusted mortality (OR 1.18 per 1 mL/kg PBW increase in tidal volume, CI 1.04 to 1.35, p = 0.010). We observed no association between driving pressure or respiratory compliance and mortality in patients without ARDS. In ARDS patients, both ΔP (OR1.1, CI 1.06-1.14, p < 0.001) and tidal volume (OR 1.17, CI 1.04-1.31, p = 0.007) were associated with mortality.
In a large retrospective analysis of critically ill non-ARDS patients receiving mechanical ventilation, we found that tidal volume was associated with 30-day mortality, while driving pressure was not.
在急性呼吸窘迫综合征(ARDS)患者中,小潮气量通气与死亡率降低相关。驱动压(潮气量与呼吸系统顺应性的比值)可能比潮气量更能预测 ARDS 的存活率。我们试图研究这些关联是否适用于没有 ARDS 的急性呼吸衰竭患者。
这是一项对 2 年内 12 家医院 ICU 收治的机械通气成年患者进行的回顾性队列分析。我们使用胸部 X 线报告的自然语言处理和电子病历中的数据来识别患有 ARDS 的患者。我们使用多变量逻辑回归和广义线性模型,使用急性生理学评分(APS)、Charlson 合并症指数(CCI)、年龄和 PaO/FiO 比值等协变量来估计潮气量、驱动压和呼吸系统顺应性与调整后 30 天死亡率之间的关联。
我们研究了 2641 名患者;48%(n=1273)患有 ARDS。ARDS 患者的平均 APS 更高(25 比 23,p<0.001),但 CCI 评分相似(4 比 3,p=0.6)。对于非 ARDS 患者,潮气量与调整后的死亡率增加相关(潮气量每增加 1ml/kgPBW,OR 为 1.18,95%CI 为 1.04 至 1.35,p=0.010)。我们没有观察到在没有 ARDS 的患者中,驱动压或呼吸系统顺应性与死亡率之间存在关联。在 ARDS 患者中,ΔP(OR1.1,CI 1.06-1.14,p<0.001)和潮气量(OR 1.17,CI 1.04-1.31,p=0.007)均与死亡率相关。
在一项对接受机械通气的非 ARDS 危重患者的大型回顾性分析中,我们发现潮气量与 30 天死亡率相关,而驱动压则没有。