Farrugia Alexia, Widlak Monika, Evans Charles, Smith Stephen Charles, Arasaradnam Ramesh
Department of Surgery, University Hospitals Coventry and Warwickshire NHS Trust, Coventry, UK.
Warwick Medical School, University of Warwick, Warwick Medical School, Coventry, UK.
Frontline Gastroenterol. 2020 Jan;11(1):28-33. doi: 10.1136/flgastro-2018-101174. Epub 2019 May 11.
Faecal immunochemical test (FIT) shows promise as a non-invasive triage test for colorectal cancer (CRC) in the symptomatic population. The aim of this study was to assess the use of FIT within the recent NG12 and DG30 National Institute for Health and Care Excellence (NICE) guidelines.
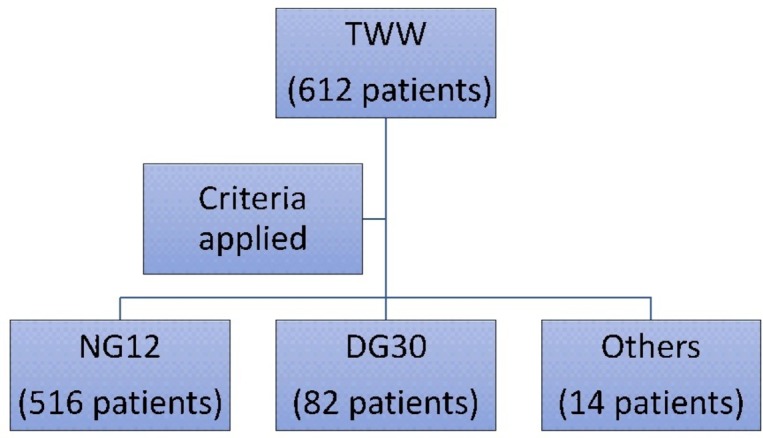
A single-centre prospective study of patients referred to University Hospitals Coventry and Warwickshire NHS Trust via the 2-week wait (TWW) pathway between January 2015 and March 2016 was conducted. 612 patients were reviewed, of which 519 were found to meet the NG12 criteria and 79 met the DG30 criteria. Data included age, sex, symptoms, colonoscopy or CT colonography, histology and FIT results.
FIT was performed in all patients and sensitivity, specificity, positive predictive value and negative predictive value, with 95% CI, for cancers and adenomas within each pathway (TWW, NG12 and DG30) was calculated.
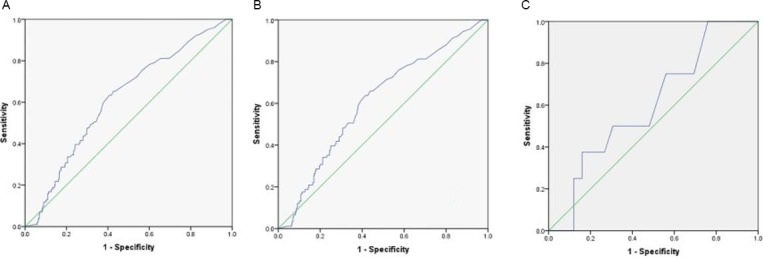
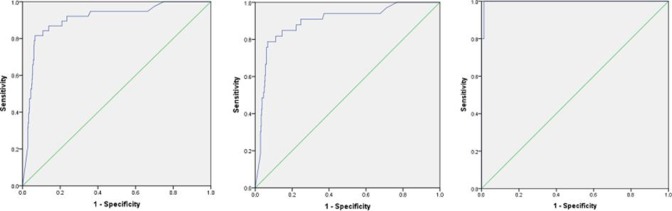
CRC sensitivity in TWW pathway patients, NG12 and DG30 group was 86.84% (95% CI 71.91% to 95.59%), 84.85% (95% CI 68.1% to 94.89%) and 100% (95% CI 47.82% to 100%), respectively. Specificity was 82.23% (95% CI 78.85% to 85.27%), 81.28% (95% CI 77.52% to 84.65%) and 91.89% (95% CI 83.18% to 96.97%), respectively. Adenoma sensitivity in the groups was 30.69% (95% CI 29.9% to 40.66%), 30.77% (95% CI 21.51% to 41.32%) and 25% (95% CI 3.19% to 65.09%), respectively.
Use of FIT within the remit of the NG12 NICE guidelines shows a high sensitivity and specificity and may be an effective triage tool when considering whether to perform investigations. However, there is still a miss rate. FIT within DG30 has excellent sensitivity and improved specificity; however, DG30 targets lower risk groups and accounts for only 13% of the entire referrals for suspected cancer. Therefore, managing the larger, higher risk NG12 group may require the addition of another test or marker to ensure that CRC is not missed.
粪便免疫化学检测(FIT)有望成为有症状人群中结直肠癌(CRC)的一种非侵入性分诊检测方法。本研究的目的是评估在最近的英国国家卫生与临床优化研究所(NICE)NG12和DG30指南范围内FIT的应用情况。
对2015年1月至2016年3月期间通过2周等待(TWW)途径转诊至考文垂大学医院和沃里克郡国民保健服务信托基金的患者进行了一项单中心前瞻性研究。对612名患者进行了评估,其中519名符合NG12标准,79名符合DG30标准。数据包括年龄、性别、症状、结肠镜检查或CT结肠成像、组织学和FIT结果。
对所有患者进行FIT检测,并计算各途径(TWW、NG12和DG30)内癌症和腺瘤的敏感性、特异性、阳性预测值和阴性预测值以及95%置信区间。
TWW途径患者、NG12组和DG30组中结直肠癌的敏感性分别为86.84%(95%置信区间71.91%至95.59%)、84.85%(95%置信区间68.1%至94.89%)和100%(95%置信区间47.82%至100%)。特异性分别为82.23%(95%置信区间78.85%至85.27%)、81.28%(95%置信区间77.52%至84.65%)和91.89%(95%置信区间83.18%至96.97%)。各组中腺瘤的敏感性分别为30.69%(95%置信区间29.9%至40.66%)、30.77%(95%置信区间21.51%至41.32%)和25%(95%置信区间3.19%至65.09%)。
在NG12 NICE指南范围内使用FIT显示出高敏感性和特异性,在考虑是否进行检查时可能是一种有效的分诊工具。然而,仍有漏诊率。DG30范围内的FIT具有出色的敏感性和提高的特异性;然而,DG30针对的是低风险人群,仅占所有疑似癌症转诊病例的13%。因此,管理规模更大、风险更高的NG12组可能需要增加另一项检测或标志物,以确保不遗漏结直肠癌。