Ito Takashi, Totoki Takaaki, Yokoyama Yayoi, Yasuda Tomotsugu, Furubeppu Hiroaki, Yamada Shingo, Maruyama Ikuro, Kakihana Yasuyuki
1Department of Emergency and Intensive Care Medicine, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan.
2Department of Systems Biology in Thromboregulation, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan.
J Intensive Care. 2019 Dec 26;7:63. doi: 10.1186/s40560-019-0420-2. eCollection 2019.
Recent studies have suggested that anticoagulant therapy does not confer a survival benefit overall in sepsis, but might be beneficial in sepsis-associated disseminated intravascular coagulation (DIC). In particular, those with high Sequential Organ Failure Assessment (SOFA) scores might be the optimal target for anticoagulant therapy. However, both DIC and SOFA scores require the measurement of multiple markers. The purpose of this study was to explore a minimal marker set for determining coagulopathy at high risk of death in septic patients, wherein histone H3 levels were evaluated as indicators of both organ failure and coagulation activation.
We analyzed correlations among levels of serum histone H3 and other coagulation markers in 85 cases of sepsis using Spearman's rank correlation test. We then compared the utility of histone H3 to that of other coagulation markers in predicting the traditional DIC state or 28-day mortality by receiver-operating characteristics analysis. Finally, we suggested cut-off values for determining coagulopathy with high risk of death, and evaluated their prognostic utility.
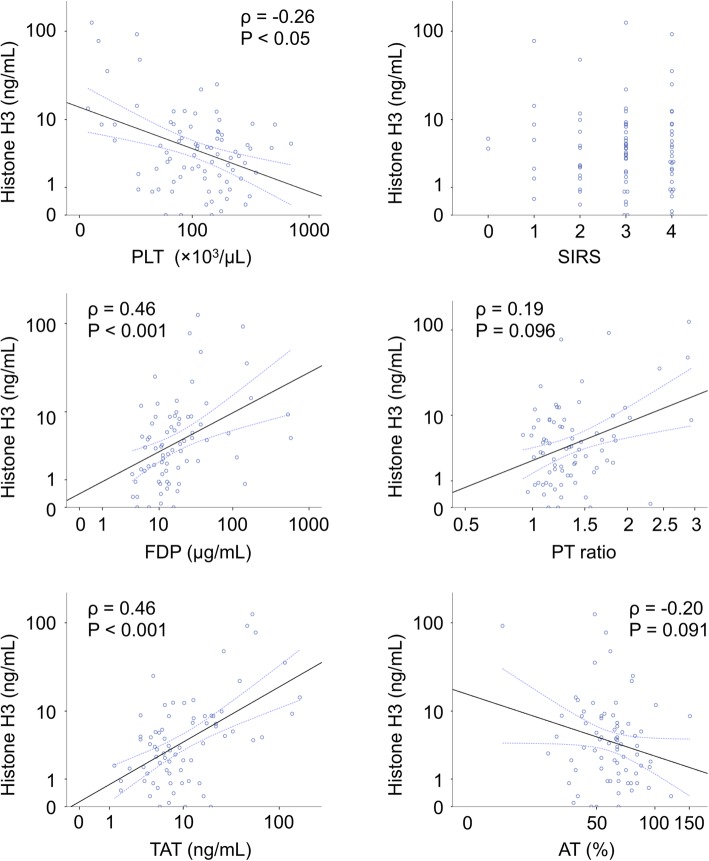
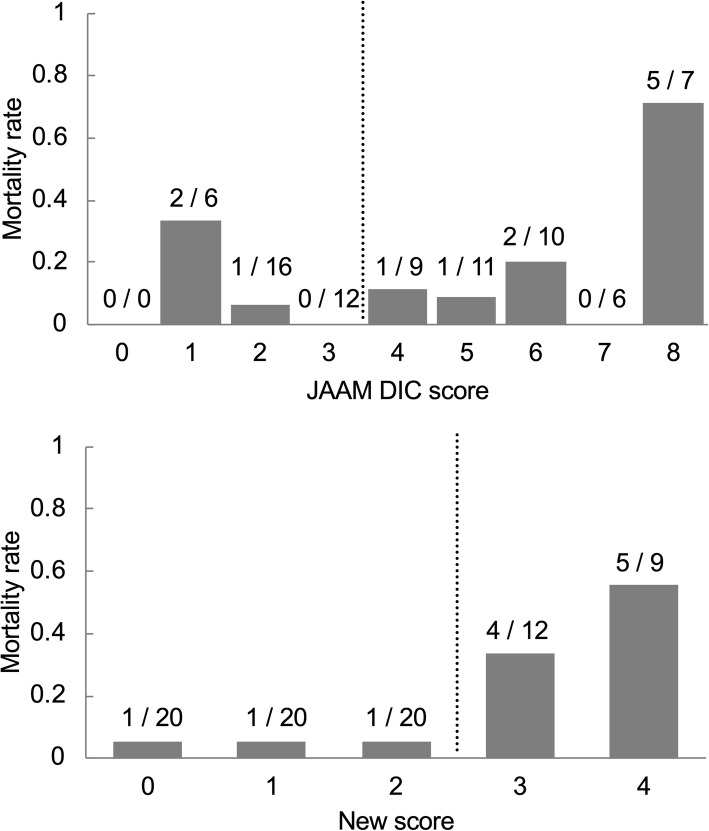
Serum histone H3 levels significantly correlated with thrombin-antithrombin complex (TAT) levels (Spearman's ρ = 0.46, < 0.001), and weakly correlated with platelet counts (Spearman's ρ = - 0.26, < 0.05). Compared to other coagulation markers, histone H3 levels showed better performance in predicting 28-day mortality. When combining serum histone H3 levels with platelet counts, our new scoring system showed a concordance rate of 69% with the traditional four-factor criteria of DIC established by the Japanese Association for Acute Medicine. The 28-day mortality rates of the new and the traditional criteria-positive patients were 43% and 21%, respectively. Those of the new and the traditional criteria-negative patients were 5.7% and 9.4%, respectively.
Serum histone H3 levels and platelet counts are potential markers for determining coagulopathy with high risk of death in septic patients. Further studies are needed to clarify the utility of serum histone H3 levels in the diagnostic of coagulopathy/DIC.
近期研究表明,抗凝治疗总体上并未给脓毒症患者带来生存获益,但可能有益于脓毒症相关的弥散性血管内凝血(DIC)。特别是,序贯器官衰竭评估(SOFA)评分高的患者可能是抗凝治疗的最佳目标。然而,DIC和SOFA评分都需要测量多个指标。本研究的目的是探索一套最小的指标集,用于确定脓毒症患者中死亡高风险的凝血病,其中组蛋白H3水平被评估为器官衰竭和凝血激活的指标。
我们使用Spearman等级相关检验分析了85例脓毒症患者血清组蛋白H3水平与其他凝血指标之间的相关性。然后,通过受试者工作特征分析,比较了组蛋白H3与其他凝血指标在预测传统DIC状态或28天死亡率方面的效用。最后,我们提出了用于确定死亡高风险凝血病的临界值,并评估了它们的预后效用。
血清组蛋白H3水平与凝血酶 - 抗凝血酶复合物(TAT)水平显著相关(Spearman's ρ = 0.46,P < 0.001),与血小板计数弱相关(Spearman's ρ = - 0.26,P < 0.05)。与其他凝血指标相比,组蛋白H3水平在预测28天死亡率方面表现更好。当将血清组蛋白H3水平与血小板计数相结合时,我们的新评分系统与日本急性医学协会制定的传统DIC四因素标准的符合率为69%。新标准阳性和传统标准阳性患者的28天死亡率分别为43%和21%。新标准阴性和传统标准阴性患者的28天死亡率分别为5.7%和9.4%。
血清组蛋白H3水平和血小板计数是确定脓毒症患者死亡高风险凝血病的潜在指标。需要进一步研究以阐明血清组蛋白H3水平在凝血病/DIC诊断中的效用。