Department of Sociology and Demography Unit, Stockholm University, S-106 91, Stockholm, Sweden.
BMC Public Health. 2020 Jan 6;20(1):8. doi: 10.1186/s12889-019-8103-4.
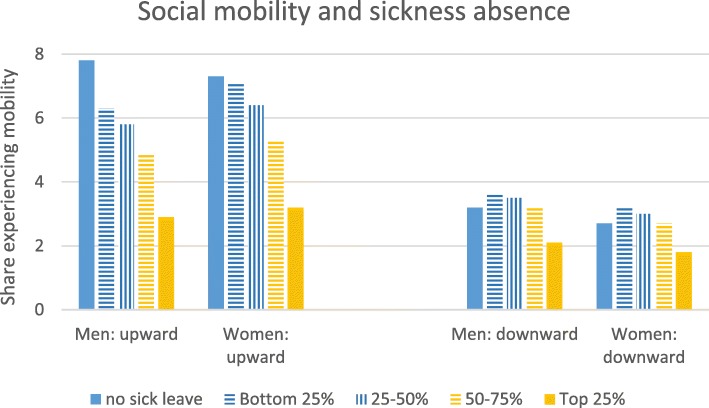
Poor health could influence how individuals are sorted into occupational classes. Health selection has therefore been considered a potential modifier to the mortality class gradient through differences in social mobility. Direct health selection in particular may operate in the short-term as poor health may lead to reduced work hours or achievement, downward social mobility, unemployment or restricted upward mobility, and death. In this study, the relationship between social mobility and mortality (all-cause, cancer-related, cardiovascular disease-related (CVD), and suicide) is explored when the relationship is adjusted for poor health.
Using Swedish register data (1996-2012) and discrete time event-history analysis, odds ratios and average marginal effects (AME) of social mobility and unemployment on mortality are observed before and after accounting for sickness absence in the previous year.
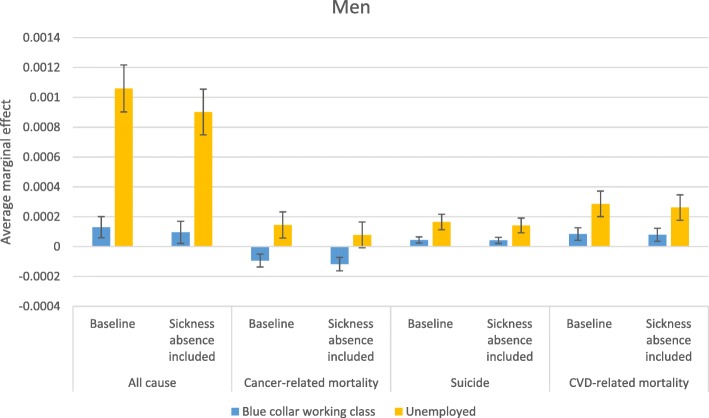
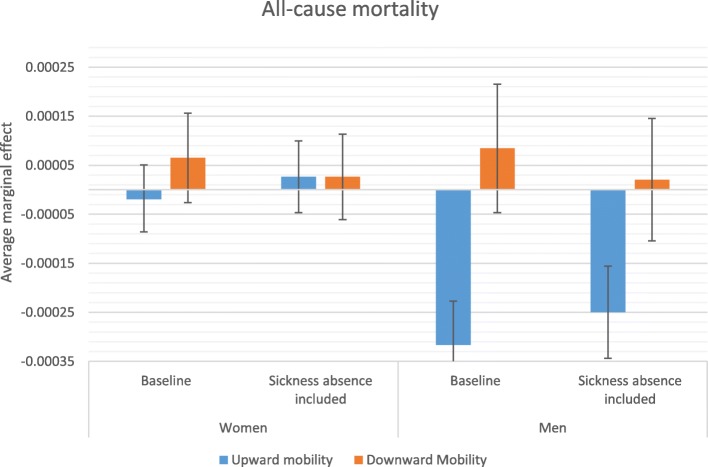
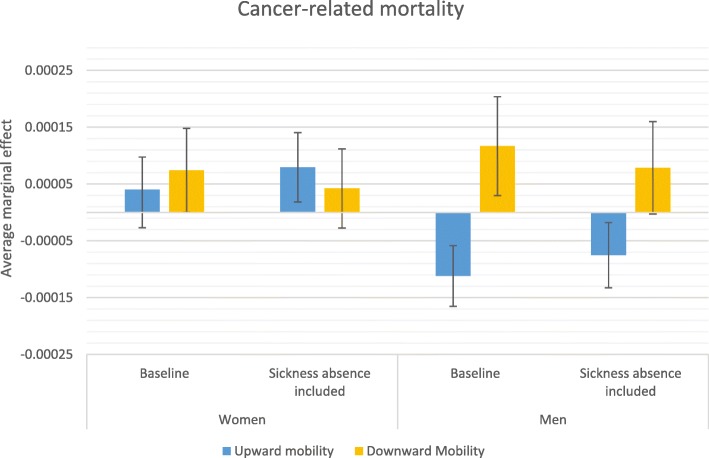
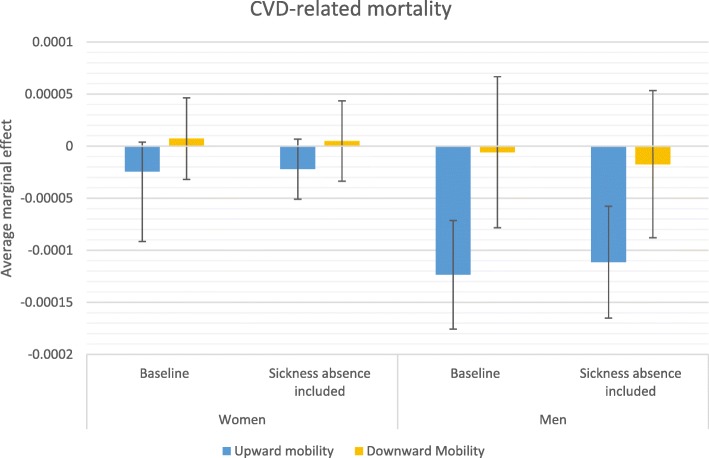
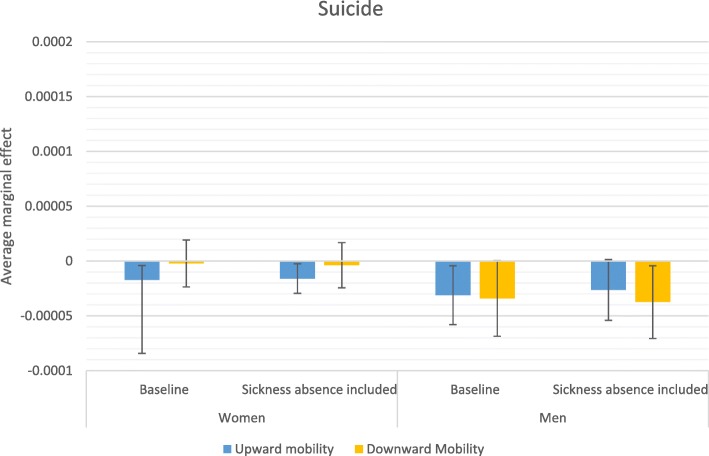
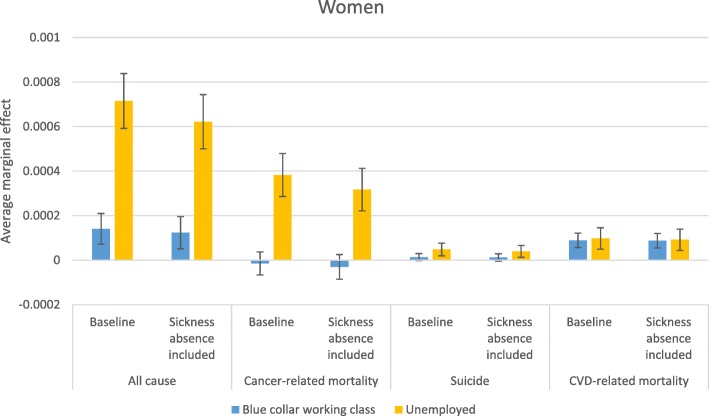
After adjusting for sickness absence, all-cause mortality remained lower for men after upward mobility in comparison to not being mobile (OR 0.82, AME -0.0003, CI - 0.0003 to - 0.0002). Similarly, upward mobility continued to be associated with lower cancer-related mortality for men (OR 0.85, AME -0.00008, CI - 0.00002 to - 0.0002), CVD-related mortality for men (OR 0.76, AME -0.0001, CI - 0.00006 to - 0.0002) and suicide for women (OR 0.67, AME -0.00002, CI - 0.000002 to - 0.00003). The relationship between unemployment and mortality also persisted across most causes of death for both men and women after controlling for previous sickness absence. In contrast, adjusting for sickness absence renders the relationship between downward mobility and cancer-related mortality not statistically different from the non-mobile.
Health selection plays a role in how downward mobility is linked to cancer related deaths. It additionally accounts for a portion of why upward mobility is associated with lower mortality. That health selection plays a role in how social mobility and mortality are related may be unexpected in a context with strong job protection. Job protection does not, however, equalize opportunities for upward mobility, which may be limited for those who have been ill. Because intra-generational upward mobility and mortality remained related after adjusting for sickness absence, other important mechanisms such as indirect selection or social causation should be explored.
健康状况不佳可能会影响个体在职业类别中的分配。因此,健康选择被认为是通过社会流动性差异影响死亡率阶层梯度的一个潜在调节因素。特别是直接的健康选择可能会在短期内起作用,因为健康状况不佳可能导致工作时间减少或成绩下降、社会地位下降、失业或向上流动受限以及死亡。在这项研究中,当调整健康状况时,探讨了社会流动性与死亡率(全因、癌症相关、心血管疾病相关(CVD)和自杀)之间的关系。
使用瑞典登记数据(1996-2012 年)和离散时间事件历史分析,观察了在考虑前一年病假的情况下,社会流动性和失业对死亡率的比值比和平均边际效应(AME)。
调整病假后,与没有流动性相比,男性向上流动后的全因死亡率仍然较低(OR 0.82,AME-0.0003,CI-0.0003 至-0.0002)。同样,男性向上流动与癌症相关死亡率降低(OR 0.85,AME-0.00008,CI-0.00002 至-0.0002)、男性 CVD 相关死亡率降低(OR 0.76,AME-0.0001,CI-0.00006 至-0.0002)和女性自杀率降低(OR 0.67,AME-0.00002,CI-0.000002 至-0.00003)相关。在控制了前一年的病假后,男性和女性的失业与死亡率之间的关系也在大多数死因中持续存在。相比之下,调整病假后,向下流动与癌症相关死亡率之间的关系与非流动性没有统计学差异。
健康选择在向下流动与癌症相关死亡之间的关系中起着作用。此外,它还解释了为什么向上流动与较低的死亡率有关的一部分原因。在具有强大工作保护的背景下,健康选择在社会流动性和死亡率之间的关系中起作用可能是出乎意料的。然而,工作保护并不能平等地为向上流动创造机会,对于那些生病的人来说,机会可能是有限的。由于在调整病假后,代际向上流动和死亡率仍然相关,因此应该探索其他重要机制,如间接选择或社会因果关系。