Department of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Department of Health Services Research, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Ann Surg Oncol. 2020 Apr;27(4):1013-1022. doi: 10.1245/s10434-019-08165-2. Epub 2020 Jan 8.
The effect of surgeon factors on patient-reported quality-of-life outcomes after breast-conserving therapy (BCT) is unknown and may help patients make informed care decisions.
We performed a survey study of women aged ≥ 67 years with non-metastatic breast cancer diagnosed in 2009 and treated with guideline-concordant BCT, to determine the association of surgeon factors with patient-reported outcomes. The treating surgeon was identified using Medicare claims, and surgeon factors were identified via the American Medical Association Physician Masterfile. The primary outcome was patient-reported cosmetic satisfaction measured by the Cancer Surveillance and Outcomes Research Team (CanSORT) Satisfaction with Breast Cosmetic Outcome instrument, while secondary outcomes included BREAST-Q subdomains. All patient, treatment, and surgeon covariables were included in a saturated multivariable linear regression model with backward elimination applied until remaining variables were p < 0.1.
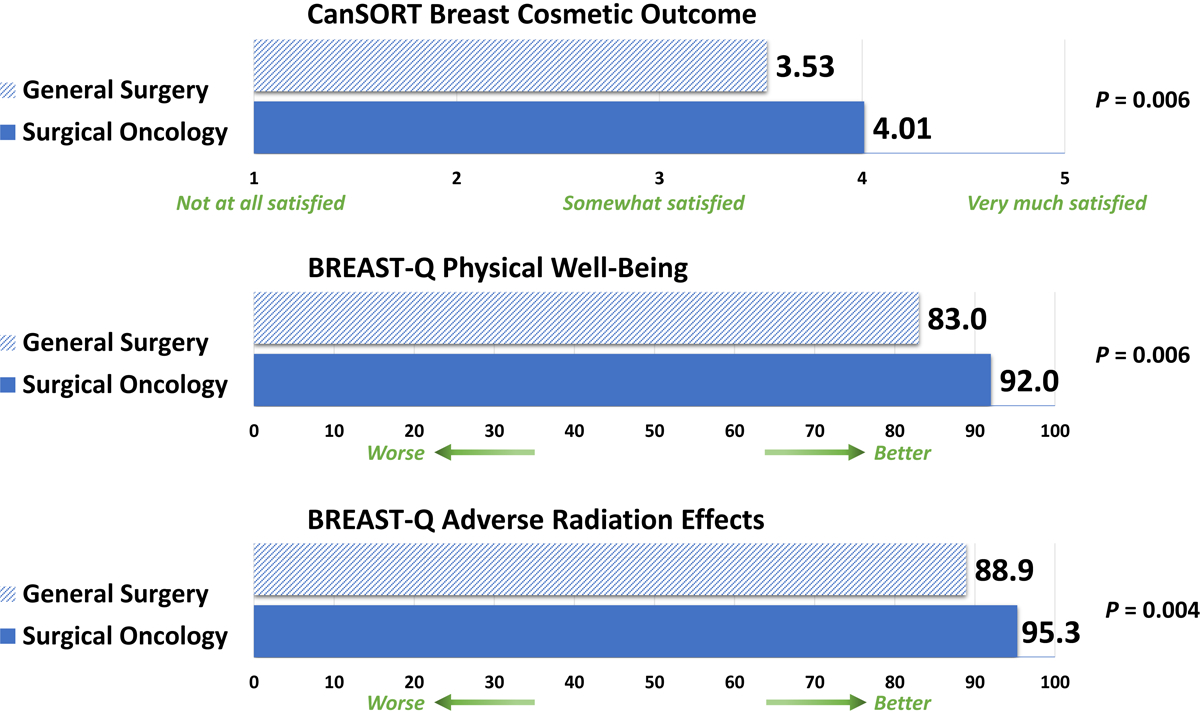
Of 1650 women randomly selected to receive the questionnaire, 489 responded, of whom 289 underwent BCT. Median age at diagnosis was 72 years and the time from diagnosis to survey was 6 years. The mean adjusted CanSORT score was higher for patients treated by surgical oncologists than patients treated by non-surgical oncologists (4.01 [95% confidence interval [CI] 3.65-4.38] vs. 3.53 [95% CI 3.28-3.77], p = 0.006). Similarly, mean adjusted BREAST-Q Physical Well-Being (91.97 [95% CI 86.13-97.80] vs. 83.04 [95% CI 80.85-85.22], p = 0.006) and Adverse Radiation Effects (95.28 [95% CI 91.25-99.31] vs. 88.90 [95% CI 86.23-91.57], p = 0.004) scores were better among patients treated by surgical oncologists.
Specialized surgical oncology training is associated with improved long-term patient-reported outcomes. These findings underscore the value of specialized training and may be useful to patients choosing their care team.
外科医生因素对保乳治疗(BCT)后患者报告的生活质量结果的影响尚不清楚,这可能有助于患者做出明智的治疗决策。
我们对 2009 年诊断为非转移性乳腺癌且接受符合指南的 BCT 治疗的年龄≥67 岁的女性进行了一项问卷调查研究,以确定外科医生因素与患者报告的结果之间的关联。使用医疗保险索赔确定治疗外科医生,使用美国医学协会医师主文件确定外科医生因素。主要结局是通过癌症监测和结果研究团队(CanSORT)的乳房美容结局满意度量表(Cosmetic Satisfaction with Breast Cosmetic Outcome instrument)测量的患者报告的美容满意度,次要结局包括 BREAST-Q 子域。所有患者、治疗和外科医生的协变量均包含在一个饱和的多变量线性回归模型中,采用向后消除法,直到剩余变量的 p 值<0.1。
在随机选择的 1650 名女性中,有 489 名女性回复了问卷,其中 289 名女性接受了 BCT。诊断时的中位年龄为 72 岁,从诊断到调查的时间为 6 年。接受外科肿瘤学家治疗的患者的平均调整后 CanSORT 评分高于接受非外科肿瘤学家治疗的患者(4.01[95%置信区间(CI)3.65-4.38]与 3.53[95% CI 3.28-3.77],p=0.006)。同样,接受外科肿瘤学家治疗的患者的平均调整后 BREAST-Q 身体整体健康状况(91.97[95% CI 86.13-97.80]与 83.04[95% CI 80.85-85.22],p=0.006)和不良放射效应(95.28[95% CI 91.25-99.31]与 88.90[95% CI 86.23-91.57],p=0.004)评分也更好。
专门的外科肿瘤学培训与改善长期患者报告的结果有关。这些发现强调了专门培训的价值,可能对选择治疗团队的患者有用。