Xie Li, Xia Leizhou, Klaiber Ulla, Sachsenmaier Milena, Hinz Ulf, Bergmann Frank, Strobel Oliver, Büchler Markus W, Neoptolemos John P, Fortunato Franco, Hackert Thilo
Department of General, Visceral and Transplantation Surgery, University Clinic, Heidelberg, Germany.
Section Surgical Research, University Clinic, Heidelberg, Germany.
Oncotarget. 2019 Dec 31;10(68):7276-7287. doi: 10.18632/oncotarget.27399.
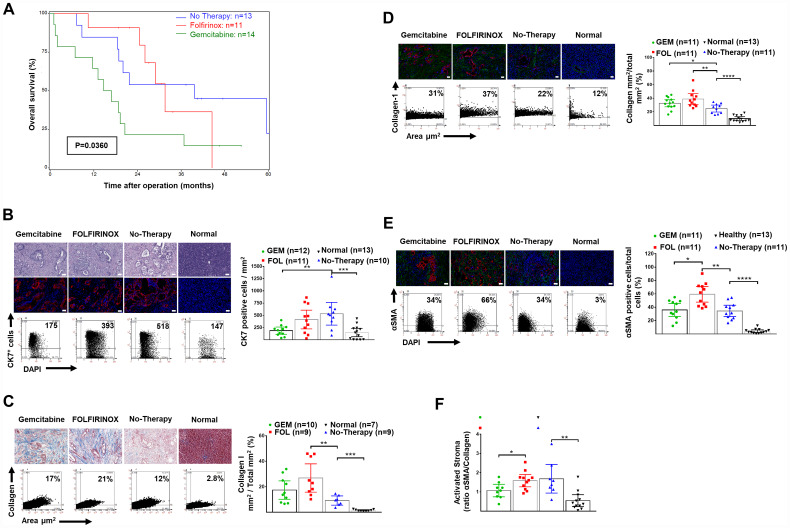
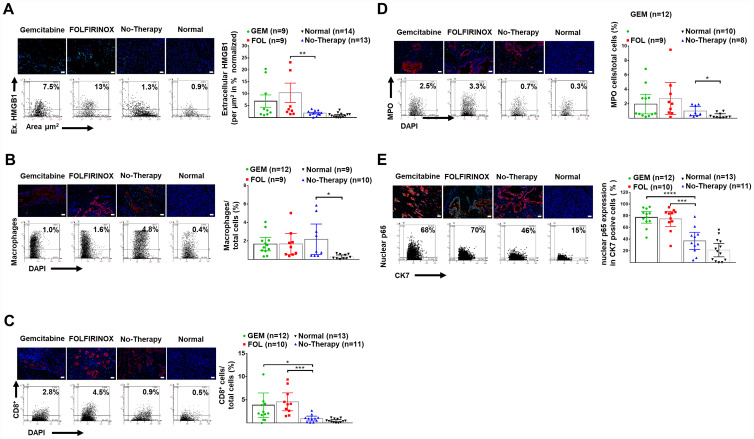
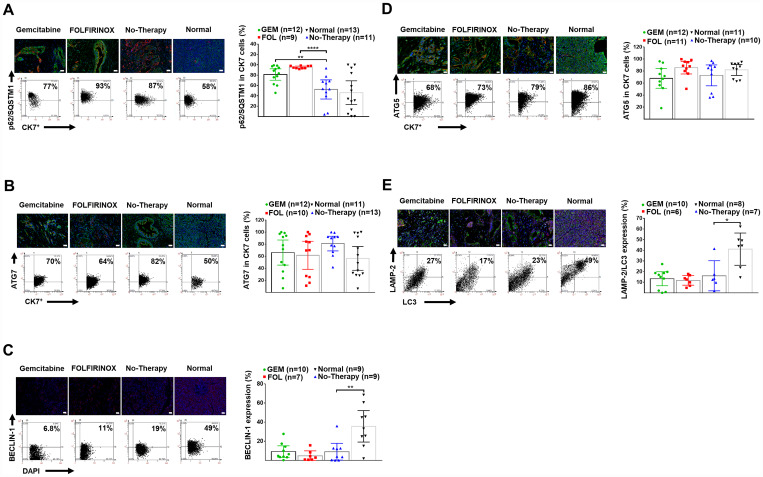
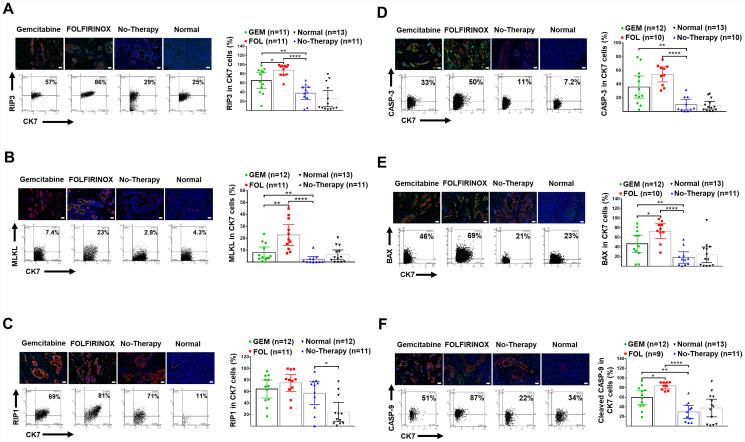
The progression and response to systemic treatment of cancer is substantially dependent on the balance between cancer cell death (apoptosis and necroptosis) and cancer cell survival (autophagy). Although well characterized in experimental systems, the status of cancer cell survival and cell death in human pancreatic ductal adenocarcinoma (PDAC), especially in response to chemotherapy and different types of chemotherapy is poorly described. The median (95% confidence interval) survival was 31.6 (24.5-44.5) months after FOLFIRINOX versus 15.8 (2.0-20.5) months after gemcitabine-based therapy ( = 0.039). PDAC tissue autophagy was reduced compared to normal pancreata based on reduced BECLIN-1 expression and LC3-Lamp-2 colocalization, whilst necroptosis (RIP-1) was increased. Neoadjuvant therapy was associated with further reduced autophagy based on p62/SQSTM-1 accumulation, and increased necroptosis (RIP3 and pMLKL) and apoptosis (BAX, cleaved CASPASE-9 and CASPASE-3) markers, increased nuclear p65 (NF-κB) and extracellular HMGB1 expression, with greater CD8 lymphocyte infiltration. Survival was associated with reduced autophagy and increased apoptosis. Necroptosis (RIP-3, pMLKL) and apoptosis (BAX and cleaved CASPASE-9) markers were higher after FOLFIRINOX than gemcitabine-based treatment. Cancer cell autophagy, apoptosis, and necroptosis marker expression was compared in pancreatic tissue samples from 51 subjects, comprising four groups: (1) surgical resection for PDAC after FOLFIRINOX ( = 11), or (2) after gemcitabine-based ( = 14) neoadjuvant therapy, (3) patients undergoing PDAC resection without prior chemotherapy ( = 13), and (4) normal pancreata from 13 organ donors. Marker expression was undertaken using semi-automated immunofluorescence-FACS-like analysis, defining PDAC cells by CK-7 expression.
癌症的进展以及对全身治疗的反应在很大程度上取决于癌细胞死亡(凋亡和坏死性凋亡)与癌细胞存活(自噬)之间的平衡。尽管在实验系统中已有充分描述,但人类胰腺导管腺癌(PDAC)中癌细胞存活和细胞死亡的状态,尤其是对化疗和不同类型化疗的反应,却鲜有报道。接受FOLFIRINOX方案治疗后的中位(95%置信区间)生存期为31.6(24.5 - 44.5)个月,而接受吉西他滨为主的治疗后的中位生存期为15.8(2.0 - 20.5)个月(P = 0.039)。与正常胰腺相比,基于BECLIN - 1表达降低和LC3 - Lamp - 2共定位,PDAC组织中的自噬减少,而坏死性凋亡(RIP - 1)增加。新辅助治疗与基于p62/SQSTM - 内积累的自噬进一步减少、坏死性凋亡(RIP3和pMLKL)及凋亡(BAX、裂解的CASPASE - 9和CASPASE - 3)标志物增加、核p65(NF - κB)和细胞外HMGB1表达增加以及CD8淋巴细胞浸润增多相关。生存期与自噬减少和凋亡增加相关。FOLFIRINOX方案治疗后坏死性凋亡(RIP - 3、pMLKL)和凋亡(BAX和裂解的CASPASE - 9)标志物高于吉西他滨为主的治疗。在51名受试者的胰腺组织样本中比较了癌细胞自噬、凋亡和坏死性凋亡标志物的表达,这些样本分为四组:(1)FOLFIRINOX方案治疗后接受PDAC手术切除的患者(n = 11),或(2)接受吉西他滨为主(n = 14)新辅助治疗后的患者,(3)未接受过化疗的PDAC切除患者(n = 13),以及(4)来自13名器官捐赠者的正常胰腺。使用半自动免疫荧光 - 类似流式细胞术分析进行标志物表达检测,通过CK - 7表达定义PDAC细胞。