Violence Prevention Research Program, Department of Emergency Medicine, University of California Davis School of Medicine, Sacramento.
Network for Public Health Law, Los Angeles, California.
JAMA Netw Open. 2020 Jan 3;3(1):e1919066. doi: 10.1001/jamanetworkopen.2019.19066.
The Patient Protection and Affordable Care Act (ACA) permits states to expand Medicaid coverage for most low-income adults to 138% of the federal poverty level and requires the provision of mental health and substance use disorder services on parity with other medical and surgical services. Uptake of substance use disorder services with medications for opioid use disorder has increased more in Medicaid expansion states than in nonexpansion states, but whether ACA-related Medicaid expansion is associated with county-level opioid overdose mortality has not been examined.
To examine whether Medicaid expansion is associated with county × year counts of opioid overdose deaths overall and by class of opioid.
DESIGN, SETTING, AND PARTICIPANTS: This serial cross-sectional study used data from 3109 counties within 49 states and the District of Columbia from January 1, 2001, to December 31, 2017 (N = 3109 counties × 17 years = 52 853 county-years). Overdose deaths were modeled using hierarchical Bayesian Poisson models. Analyses were performed from April 1, 2018, to July 31, 2019.
The primary exposure was state adoption of Medicaid expansion under the ACA, measured as the proportion of each calendar year during which a given state had Medicaid expansion in effect. By the end of study observation in 2017, a total of 32 states and the District of Columbia had expanded Medicaid eligibility.
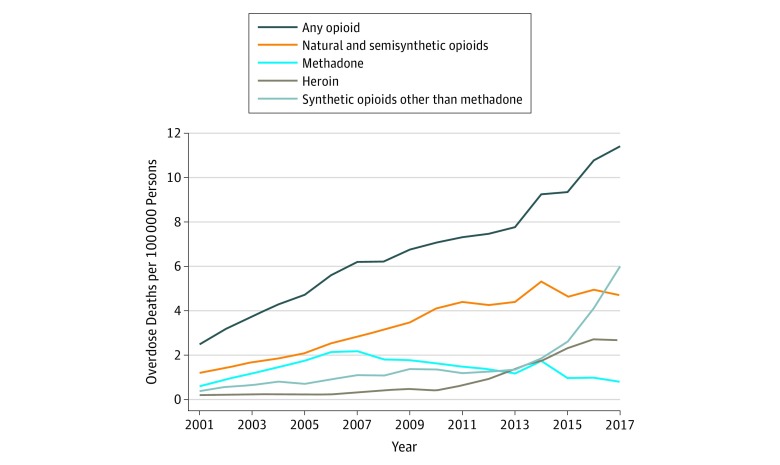
The outcomes of interest were annual county-level mortality from overdoses involving any opioid, natural and semisynthetic opioids, methadone, heroin, and synthetic opioids other than methadone, derived from the National Vital Statistics System multiple-cause-of-death files. A secondary analysis examined fatal overdoses involving all drugs.
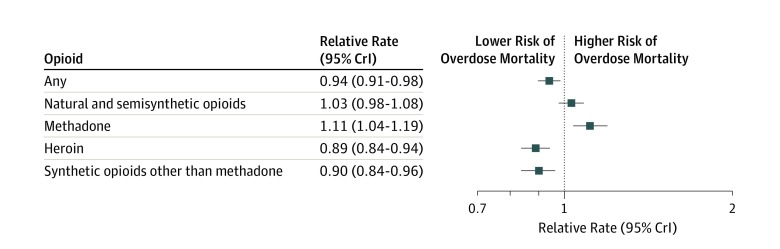
There were 383 091 opioid overdose fatalities across observed US counties during the study period, with a mean (SD) of 7.25 (27.45) deaths per county (range, 0-1145 deaths per county). Adoption of Medicaid expansion was associated with a 6% lower rate of total opioid overdose deaths compared with the rate in nonexpansion states (relative rate [RR], 0.94; 95% credible interval [CrI], 0.91-0.98). Counties in expansion states had an 11% lower rate of death involving heroin (RR, 0.89; 95% CrI, 0.84-0.94) and a 10% lower rate of death involving synthetic opioids other than methadone (RR, 0.90; 95% CrI, 0.84-0.96) compared with counties in nonexpansion states. An 11% increase was observed in methadone-related overdose mortality in expansion states (RR, 1.11; 95% CrI, 1.04-1.19). An association between Medicaid expansion and deaths involving natural and semisynthetic opioids was not well supported (RR, 1.03; 95% CrI, 0.98-1.08).
Medicaid expansion was associated with reductions in total opioid overdose deaths, particularly deaths involving heroin and synthetic opioids other than methadone, but increases in methadone-related mortality. As states invest more resources in addressing the opioid overdose epidemic, attention should be paid to the role that Medicaid expansion may play in reducing opioid overdose mortality, in part through greater access to medications for opioid use disorder.
《患者保护与平价医疗法案》(ACA)允许各州将大多数低收入成年人的医疗补助覆盖范围扩大到联邦贫困水平的 138%,并要求提供精神健康和物质使用障碍服务,与其他医疗和外科服务平等对待。在接受阿片类药物使用障碍治疗药物的物质使用障碍服务的采用率在医疗补助扩大的州比在没有扩大的州有所增加,但 ACA 相关的医疗补助扩大是否与县一级的阿片类药物过量死亡率有关尚未得到检验。
研究医疗补助扩大是否与阿片类药物总体和按阿片类药物类别计算的县一级药物过量死亡人数有关。
设计、地点和参与者:这项连续的横截面研究使用了来自 49 个州和哥伦比亚特区的 3109 个县的数据,时间为 2001 年 1 月 1 日至 2017 年 12 月 31 日(N=3109 个县×17 年=52853 个县年)。使用分层贝叶斯泊松模型对过量死亡进行建模。分析于 2018 年 4 月 1 日至 2019 年 7 月 31 日进行。
主要暴露是 ACA 下的医疗补助扩大,通过给定年份中医疗补助扩大生效的比例来衡量。到 2017 年研究观察结束时,共有 32 个州和哥伦比亚特区扩大了医疗补助资格。
感兴趣的结果是从国家生命统计系统多原因死亡文件中得出的涉及任何阿片类药物、天然和半合成阿片类药物、美沙酮、海洛因和除美沙酮以外的合成阿片类药物的年度县一级死亡率。二次分析研究了涉及所有药物的致命药物过量。
在研究期间,美国观察到的县有 383091 例阿片类药物过量死亡,平均(SD)为每县 7.25(27.45)例死亡(范围,每县 0-1145 例死亡)。与非扩大州相比,医疗补助扩大与总阿片类药物过量死亡率降低 6%相关(相对风险[RR],0.94;95%可信区间[CrI],0.91-0.98)。与非扩大州相比,扩大州的海洛因相关死亡(RR,0.89;95%CrI,0.84-0.94)和除美沙酮以外的合成阿片类药物相关死亡(RR,0.90;95%CrI,0.84-0.96)的死亡率较低。在扩大州,与美沙酮相关的过量死亡率增加了 11%(RR,1.11;95%CrI,1.04-1.19)。医疗补助扩大与涉及天然和半合成阿片类药物的死亡之间的关联没有得到很好的支持(RR,1.03;95%CrI,0.98-1.08)。
医疗补助扩大与阿片类药物总过量死亡人数的减少有关,特别是与海洛因和除美沙酮以外的合成阿片类药物有关的死亡人数,但与美沙酮有关的死亡率有所增加。随着各州投入更多资源应对阿片类药物过量流行,应注意医疗补助扩大可能在减少阿片类药物过量死亡率方面所起的作用,部分原因是通过更多地获得阿片类药物使用障碍治疗药物。