Institut National de Santé Publique, Bujumbura, Burundi.
Health Economics Unit, Department of Public Health, Institute of Tropical Medicine, Antwerp, Belgium.
PLoS One. 2020 Jan 13;15(1):e0226376. doi: 10.1371/journal.pone.0226376. eCollection 2020.
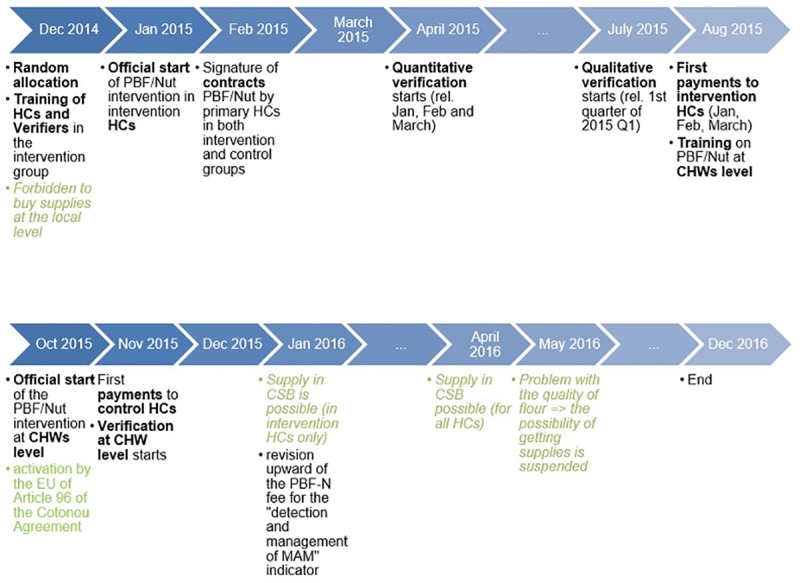
From January 2015 to December 2016, the health authorities in Burundi piloted the inclusion of child nutrition services into the pre-existing performance-based financing free health care policy (PBF-FHC). An impact evaluation, focused on health centres, found positive effects both in terms of volume of services and quality of care. To some extent, this result is puzzling given the harshness of the contextual constraints related to the fragile setting.
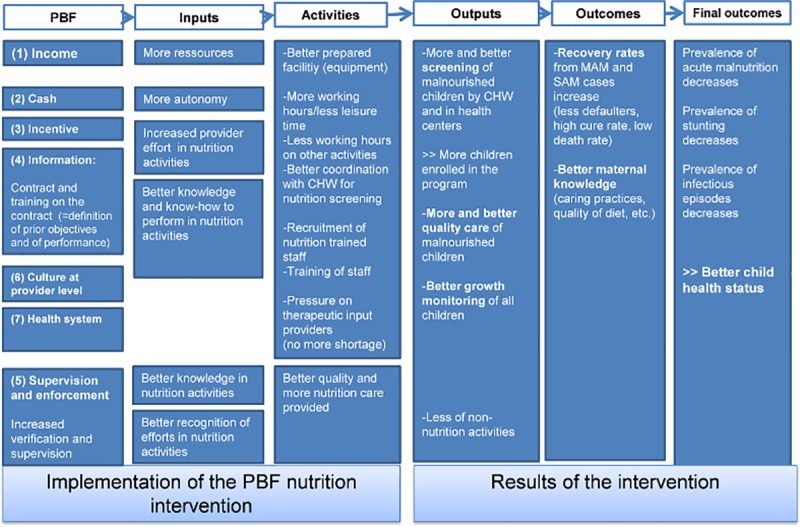
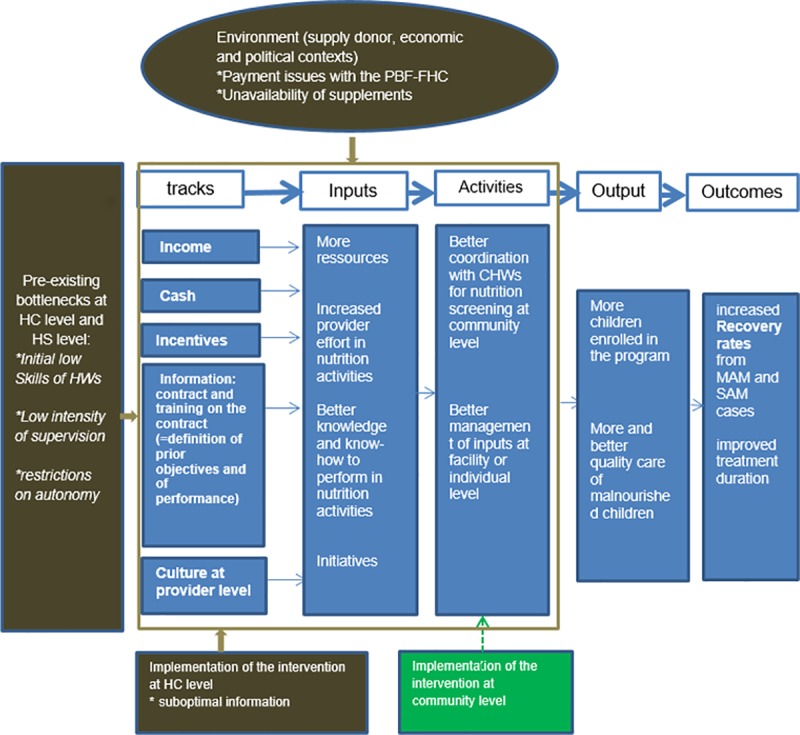
With a multi-methods approach, we explored how contextual and implementation constraints interacted with the pre-identified tracks of effect transmission embodied in the intervention. For our analysis, we used a hypothetical Theory of Change (ToC) that mapped a set of seven tracks through which the intervention might develop positive effects for children suffering from malnutrition. We built our analysis on (1) findings from the facility surveys and (2) extra qualitative data (logbooks, interviews and operational document reviews).
Our results suggest that six constraints have weighted upon the intervention: (1) initial low skills of health workers; (2) unavailability of resources (including nutritional dietary inputs and equipment); (3) payment delays; (4) suboptimal information; (5) restrictions on autonomy; and (6) low intensity of supervision. Together, they have affected the intensity of the intervention, especially during its first year. From our analysis of the ToC, we noted that the positive effects largely occurred as a result of the incentive and information tracks. Qualitative data suggests that health centres have circumvented the many constraints by relying on a community-based recruitment strategy and a better management of inputs at the level of the facility and the patient himself.
Frontline actors have agency: when incentives are right, they take the initiative and find solutions. However, they cannot perform miracles: Burundi needs a holistic societal strategy to resolve the structural problem of child malnutrition.
Clinical Trials.gov Identifier: NCT02721160; March 2016 (retrospectively registered).
从 2015 年 1 月到 2016 年 12 月,布隆迪卫生当局试行将儿童营养服务纳入现有的基于绩效的融资免费医疗保健政策(PBF-FHC)。一项以卫生中心为重点的影响评估发现,在服务量和护理质量方面都产生了积极影响。在一定程度上,鉴于与脆弱环境相关的严峻背景限制,这一结果令人费解。
我们采用多方法方法,探讨了背景和实施限制如何与干预措施中预先确定的影响传递轨迹相互作用。在我们的分析中,我们使用了一个假设的变革理论(ToC),该理论描绘了干预措施可能为营养不良儿童带来积极影响的七个轨迹。我们的分析基于(1)来自机构调查的结果和(2)额外的定性数据(日志、访谈和操作文件审查)。
我们的结果表明,有六个限制因素影响了干预措施:(1)卫生工作者的初始技能较低;(2)资源不可用(包括营养膳食投入和设备);(3)付款延迟;(4)信息不理想;(5)限制自主权;(6)监督力度低。总的来说,这些因素影响了干预措施的强度,尤其是在其第一年。从我们对 ToC 的分析中,我们注意到,积极影响主要是由于激励和信息轨迹。定性数据表明,卫生中心通过依赖社区招聘策略和更好地管理设施层面和患者自身的投入,规避了许多限制。
一线人员有能动性:当激励措施正确时,他们会主动采取行动并寻找解决方案。然而,他们无法创造奇迹:布隆迪需要一个整体的社会战略来解决儿童营养不良的结构性问题。
ClinicalTrials.gov 标识符:NCT02721160;2016 年 3 月(追溯注册)。