Institute for Maternal & Child Health, IRCCS "Burlo Garofolo", Trieste, Italy.
Local Health Unit N.2 "Marca Trevigiana", Public Health Department, Treviso, Italy.
Sci Rep. 2020 Jan 15;10(1):380. doi: 10.1038/s41598-019-57037-y.
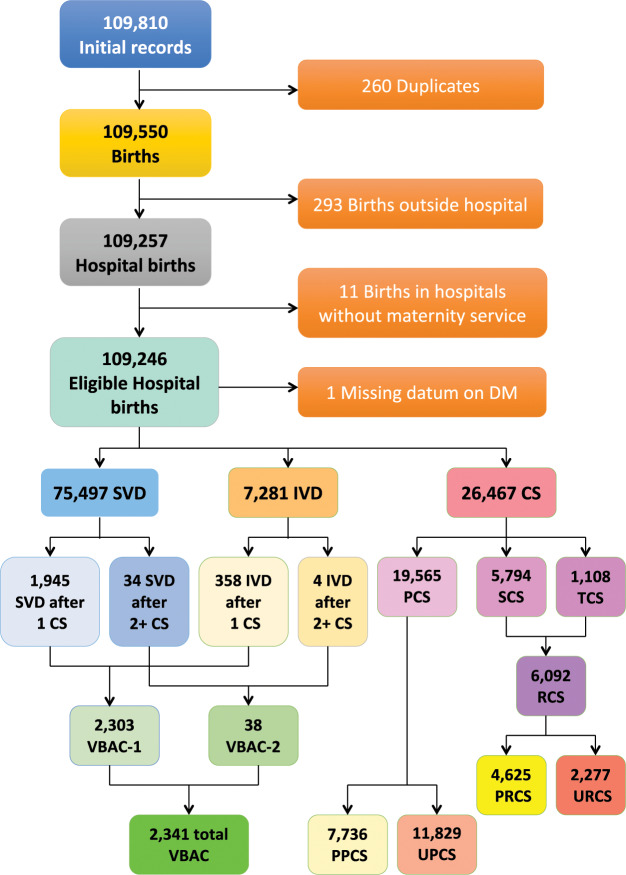
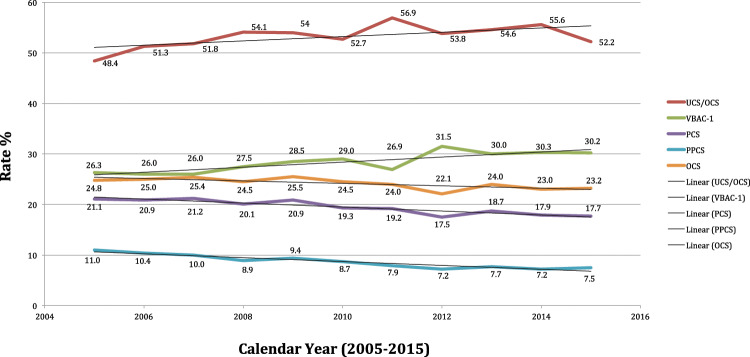
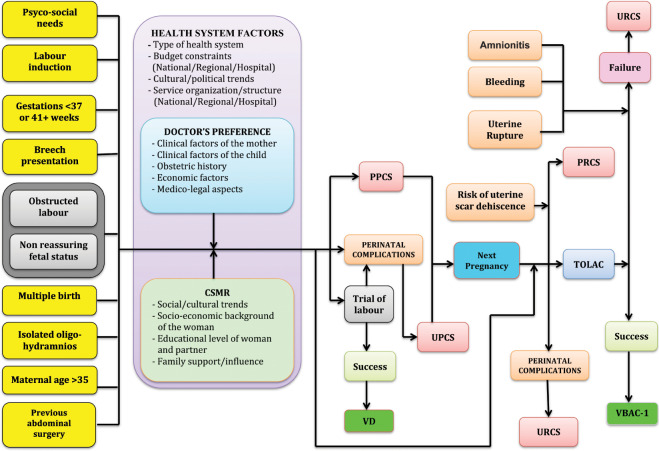
Although there is no evidence that elevated rates of cesarean sections (CS) translate into reduced maternal/child perinatal morbidity or mortality, CS have been increasingly overused almost everywhere, both in high and low-income countries. The primary cesarean section (PCS) has become a major driver of the overall CS (OCS) rate, since it carries intrinsic risk of repeat CS (RCS) in future pregnancies. In our study we examined patterns of PCS, pl compared with planned TOLAC anned PCS (PPCS), vaginal birth after 1 previous CS (VBAC-1) and associated factors in Friuli Venezia Giulia (FVG), a region of North-Eastern Italy, collecting data from its 11 maternity centres (coded from A to K) during 2005-2015. By fitting three multiple logistic regression models (one for each delivery mode), we calculated the adjusted rates of PCS and PPCS among women without history of CS, whilst the calculation of the VBAC rate was restricted to women with just one previous CS (VBAC-1). Results, expressed as odds ratio (OR) with 95% confidence interval (95%CI), were controlled for the effect of hospital, calendar year as well as several factors related to the clinical and obstetric conditions of the mothers and the newborn, the obstetric history and socio-demographic background. In FVG during 2005-2015 there were 24,467 OCS (rate of 24.2%), 19,565 PCS (19.6%), 7,736 PPCS (7.7%) and 2,303 VBAC-1 (28.4%). We found high variability of delivery mode (DM) at hospital level, especially for PCS and PPCS. Breech presentation was the strongest determinant for PCS as well as PPCS. Leaving aside placenta previa/abuptio placenta/ante-partum hemorrhage, further significant factors, more importantly associated with PCS than PPCS were non-reassuring fetal status and obstructed labour, followed by (in order of statistical significance): multiple birth; eclampsia/pre-eclampsia; maternal age 40-44 years; placental weight 600-99 g; oligohydramios; pre-delivery LoS 3-5 days; maternal age 35-39 years; placenta weight 1,000-1,500 g; birthweight < 2,000 g; maternal age ≥ 45 years; pre-delivery LoS ≥ 6 days; mother's age 30-34 years; low birthweight (2,000-2,500 g); polyhydramnions; cord prolaspe; ≥6 US scas performed during pregnancy and pre-term gestations (33-36 weeks). Significant factors for PPCS were (in order of statistical significance): breech presentation; placenta previa/abruptio placenta/ante-partum haemorrhage; multiple birth; pre-delivery LoS ≥ 3 days; placental weight ≥ 600 g; maternal age 40-44 years; ≥6 US scans performed in pregnancy; maternal age ≥ 45 and 35-39 years; oligohydramnios; eclampsia/pre-eclampsia; mother's age 30-34 years; birthweight <2,000 g; polyhydramnios and pre-term gestation (33-36 weeks). VBAC-1 were more likely with gestation ≥ 41 weeks, placental weight <500 g and especially labour analgesia. During 2005-2015 the overall rate of PCS in FVG (19.6%) was substantially lower than the corresponding figure reported in 2010 for the entire Italy (29%) and still slightly under the most recent national PCS rate for 2017 (22.2%). The VBAC-1 rate on women with history of one previous CS in FVG was 28.4% (25.3% considering VBAC on all women with at least 1 previous CS), roughly three times the Italian national rate of 9% reported for 2017. The discrepancy between the OCS rate at country level (38.1%) and FVG's (24.2%) is therefore mainly attributable to RCS. Although there was a marginal decrease of PCS and PPCS crudes rates over time in the whole region, accompained by a progressive enhancement of the crude VBAC rate, we found remarkable variability of DM across hospitals. To further contain the number of unnecessary PCS and promote VBAC where appropriate, standardized obstetric protocols should be introduced and enforced at hospital level. Decision-making on PCS should be carefully scrutinized, introducing a diagnostic second opinion for all PCS, particularly for term singleton pregancies with cephalic presentation and in case of obstructed labour as well as non-reassuring fetal status, grey areas potentially affected by subjective clinical assessment. This process of change could be facilitated with education of staff/patients by opinion leaders and prenatal counseling for women and partners, although clinical audits, financial penalties and rewards to efficient maternity centres could also be considered.
尽管没有证据表明剖宫产率(CS)的升高会降低母婴围产期发病率或死亡率,但 CS 在高收入和低收入国家都被过度使用。初次剖宫产(PCS)已成为总剖宫产率(OCS)的主要驱动因素,因为它在未来妊娠中存在重复剖宫产(RCS)的内在风险。在我们的研究中,我们检查了 PCS 的模式,与计划的 TOLAC 预先安排的 PCS(PPCS)、剖宫产后 1 次分娩(VBAC-1)和相关因素进行了比较,这些数据来自意大利东北部弗留利-威尼斯朱利亚地区(FVG)的 11 个产科中心(从 A 到 K 编码),在 2005 年至 2015 年期间收集。通过拟合三个多逻辑回归模型(一个用于每种分娩方式),我们计算了没有 CS 史的妇女中 PCS 和 PPCS 的调整率,而 VBAC-1 率的计算仅限于只有一次先前 CS 的妇女。结果以比值比(OR)和 95%置信区间(95%CI)表示,控制了医院、日历年度以及与母亲和新生儿临床和产科状况、产科史和社会人口背景相关的几个因素的影响。在 2005 年至 2015 年期间,FVG 共有 24467 例 OCS(24.2%的发生率)、19565 例 PCS(19.6%)、7736 例 PPCS(7.7%)和 2303 例 VBAC-1(28.4%)。我们发现医院水平的分娩方式(DM)存在高度变异性,尤其是 PCS 和 PPCS。臀位是 PCS 和 PPCS 的最强决定因素。除前置胎盘/胎盘早剥/产前出血外,与 PPCS 相比,与 PCS 更相关的其他重要因素包括胎儿状态不佳和产程阻滞,其次是(按统计学意义顺序排列):多胎妊娠;子痫前期/子痫;母亲年龄 40-44 岁;胎盘重量 600-99g;羊水过少;产前住院 3-5 天;母亲年龄 35-39 岁;胎盘重量 1000-1500g;出生体重<2000g;母亲年龄≥45 岁;产前住院≥6 天;母亲年龄 30-34 岁;出生体重低(2000-2500g);羊水过多;脐带脱垂;妊娠期间进行≥6 次 US 扫描;早产(33-36 周)。PPCS 的显著因素按统计学意义顺序排列为:臀位;前置胎盘/胎盘早剥/产前出血;多胎妊娠;产前住院≥3 天;胎盘重量≥600g;母亲年龄 40-44 岁;妊娠期间进行≥6 次 US 扫描;母亲年龄≥45 岁和 35-39 岁;羊水过少;子痫前期/子痫;母亲年龄 30-34 岁;出生体重<2000g;羊水过多;早产(33-36 周)。如果孕龄≥41 周、胎盘重量<500g 且尤其是分娩镇痛,则 VBAC-1 的可能性更大。在 2005 年至 2015 年期间,FVG 的总体 PCS 率(19.6%)远低于 2010 年整个意大利(29%)报告的相应数字,仍略低于 2017 年最新的全国 PCS 率(22.2%)。在 FVG 有一次先前 CS 史的妇女中,VBAC-1 的发生率为 28.4%(考虑到所有至少有一次先前 CS 的妇女,VBAC-1 的发生率为 25.3%),大致是意大利 2017 年报告的全国 9%的三倍。该国水平(38.1%)和 FVG(24.2%)之间的 OCS 率差异主要归因于 RCS。尽管整个地区的 PCS 和 PPCS 粗率都有轻微下降,但 VBAC 的粗率逐渐提高,我们发现医院之间 DM 的变异性很大。为了进一步减少不必要的 PCS 数量并适当促进 VBAC,应在医院层面引入和执行标准化的产科方案。应仔细审查 PCS 的决策,对所有 PCS 引入诊断性二次意见,特别是对足月单胎妊娠、头位分娩和产程阻滞以及胎儿状态不佳的病例,以及灰色区域,这些区域可能受到主观临床评估的影响。通过意见领袖对工作人员/患者进行教育和对妇女及其伴侣进行产前咨询,可以促进这一变化过程,尽管还可以考虑临床审核、经济处罚和对高效产科中心的奖励。