Thölking Gerold, Gillhaus Nils Hendrik, Schütte-Nütgen Katharina, Pavenstädt Hermann, Koch Raphael, Suwelack Barbara, Reuter Stefan
Department of Internal Medicine and Nephrology, University Hospital of Münster Marienhospital Steinfurt, 48565 Steinfurt, Germany.
Department of Medicine D, Division of General Internal Medicine, Nephrology and Rheumatology, University Hospital of Münster, 48149 Münster, Germany.
J Clin Med. 2020 Jan 23;9(2):328. doi: 10.3390/jcm9020328.
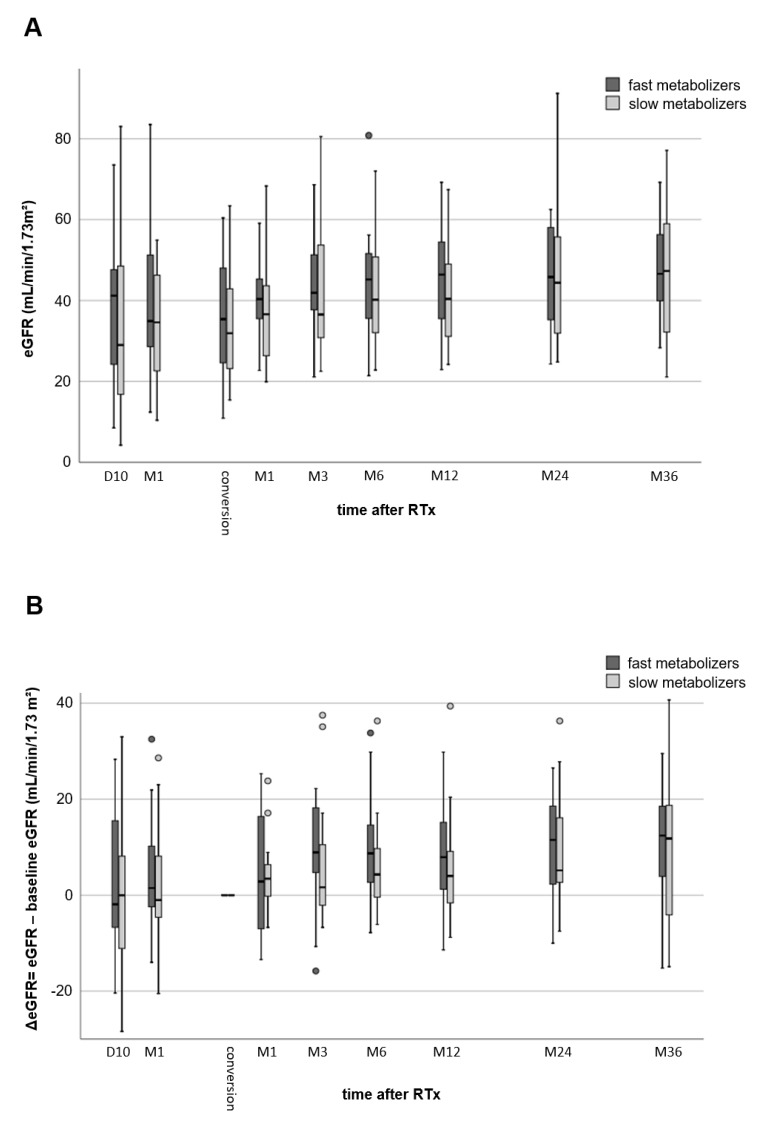
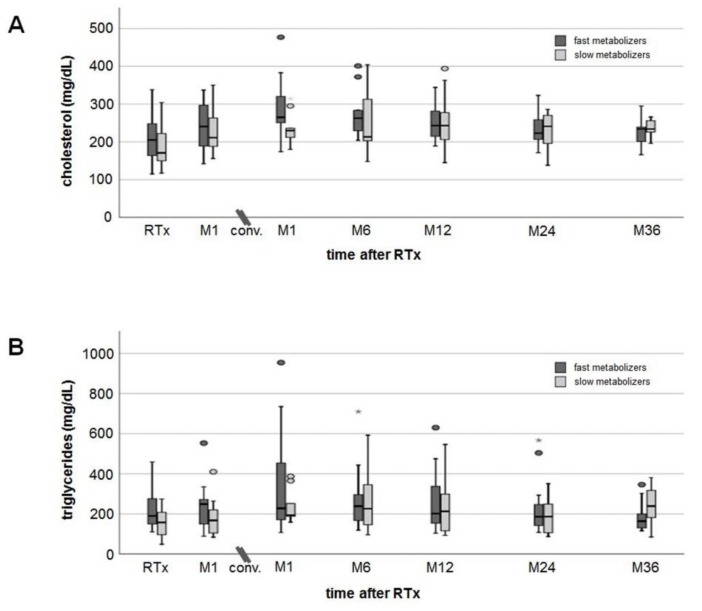
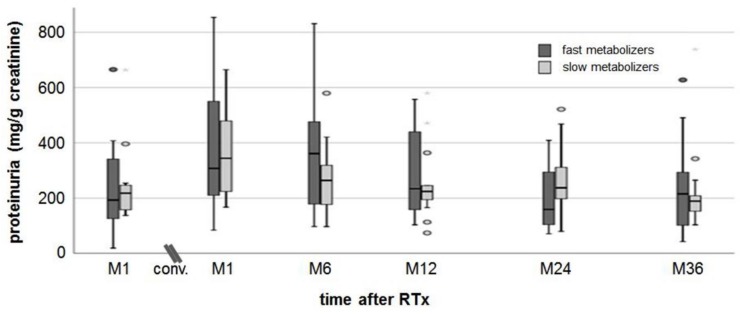
Fast tacrolimus (TAC) metabolism (concentration/dose (C/D) ratio < 1.05 ng/ml/mg) is a risk factor for inferior outcomes after renal transplantation (RTx) as it fosters, e.g., TAC-related nephrotoxicity. TAC minimization or conversion to calcineurin-inhibitor free immunosuppression are strategies to improve graft function. Hence, we hypothesized that especially patients with a low C/D ratio profit from a switch to everolimus (EVR). We analyzed data of 34 RTx recipients (17 patients with a C/D ratio < 1.05 ng/ml/mg vs. 17 patients with a C/D ratio ≥ 1.05 ng/ml/mg) who were converted to EVR within 24 months after RTx. The initial immunosuppression consisted of TAC, mycophenolate, prednisolone, and basiliximab induction. During an observation time of 36 months after changing immunosuppression from TAC to EVR, renal function, laboratory values, and adverse effects were compared between the groups. Fast TAC metabolizers were switched to EVR 4.6 (1.5-21.9) months and slow metabolizers 3.3 (1.8-23.0) months after RTx (p = 0.838). Estimated glomerular filtration rate (eGFR) did not differ between the groups at the time of conversion (baseline). Thereafter, the eGFR in all patients increased noticeably (fast metabolizers eGFR 36 months: + 11.0 ± 11.7 (p = 0.005); and slow metabolizers eGFR 36 months: + 9.4 ± 15.9 mL/min/1.73m² ( = 0.049)) vs. baseline. Adverse events were not different between the groups. After the switch, eGFR values of all patients increased statistically noticeably with a tendency towards a higher increase in fast TAC metabolizers. Since conversion to EVR was safe in a three-year follow-up for slow and fast TAC metabolizers, this could be an option to protect fast metabolizers from TAC-related issues.
他克莫司(TAC)代谢过快(浓度/剂量(C/D)比<1.05 ng/ml/mg)是肾移植(RTx)后预后较差的一个危险因素,因为它会引发例如与TAC相关的肾毒性。TAC最小化或转换为无钙调神经磷酸酶抑制剂的免疫抑制是改善移植肾功能的策略。因此,我们推测,尤其是C/D比低的患者会从转换为依维莫司(EVR)中获益。我们分析了34例RTx受者的数据(17例C/D比<1.05 ng/ml/mg的患者与17例C/D比≥1.05 ng/ml/mg的患者),这些患者在RTx后24个月内转换为EVR。初始免疫抑制包括TAC、霉酚酸酯、泼尼松龙和巴利昔单抗诱导。在将免疫抑制从TAC转换为EVR后的36个月观察期内,比较了两组患者的肾功能、实验室检查值和不良反应。快速TAC代谢者在RTx后4.6(1.5 - 21.9)个月转换为EVR,慢速代谢者在RTx后3.3(1.8 - 23.0)个月转换为EVR(p = 0.838)。转换时(基线)两组间的估计肾小球滤过率(eGFR)无差异。此后,所有患者的eGFR均显著升高(快速代谢者36个月时eGFR:+11.0±11.7(p = 0.005);慢速代谢者36个月时eGFR:+9.4±15.9 mL/min/1.73m²(p = 0.049))与基线相比。两组间不良事件无差异。转换后,所有患者的eGFR值均有统计学意义的显著升高,快速TAC代谢者升高趋势更明显。由于在三年随访中,慢速和快速TAC代谢者转换为EVR都是安全的,这可能是保护快速代谢者免受TAC相关问题影响的一种选择。