Thölking Gerold, Tosun-Koç Filiz, Jehn Ulrich, Koch Raphael, Pavenstädt Hermann, Suwelack Barbara, Reuter Stefan
Department of Internal Medicine and Nephrology, University Hospital of Münster Marienhospital Steinfurt, 48565 Steinfurt, Germany.
Department of Medicine D, Division of General Internal Medicine, Nephrology and Rheumatology, University Hospital of Münster, 48149 Münster, Germany.
J Clin Med. 2022 Feb 26;11(5):1290. doi: 10.3390/jcm11051290.
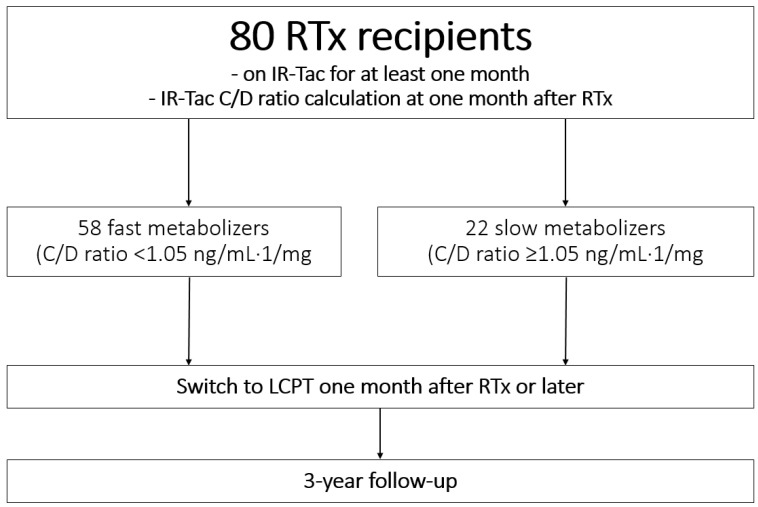
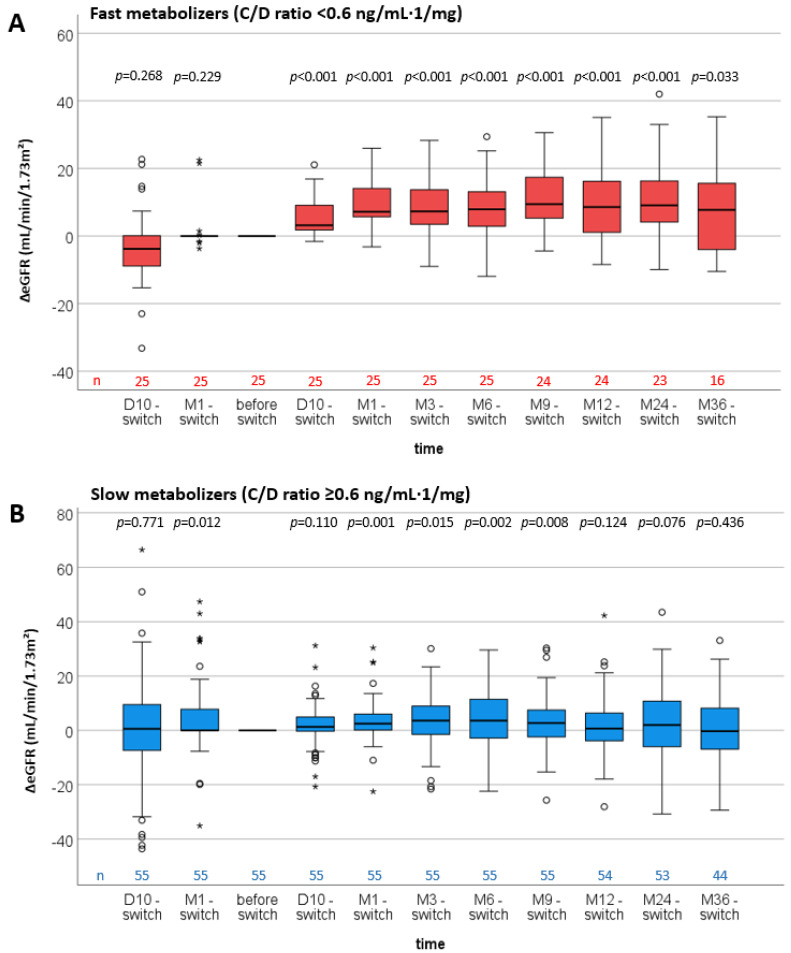
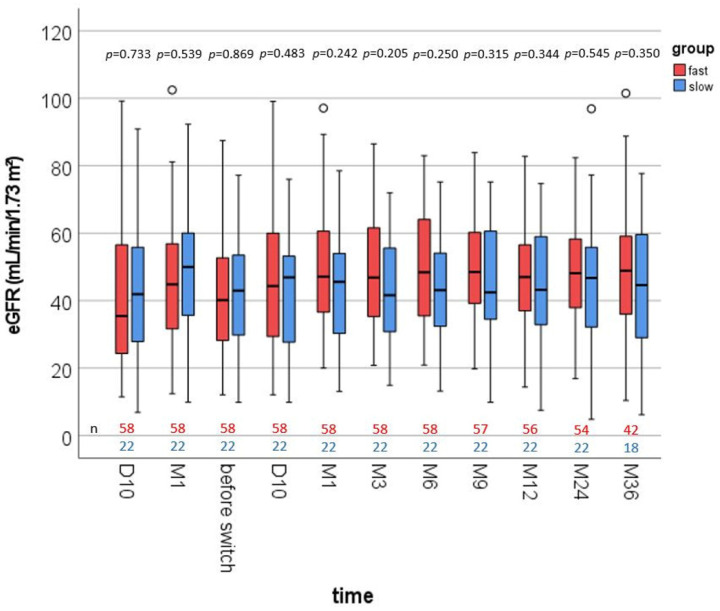
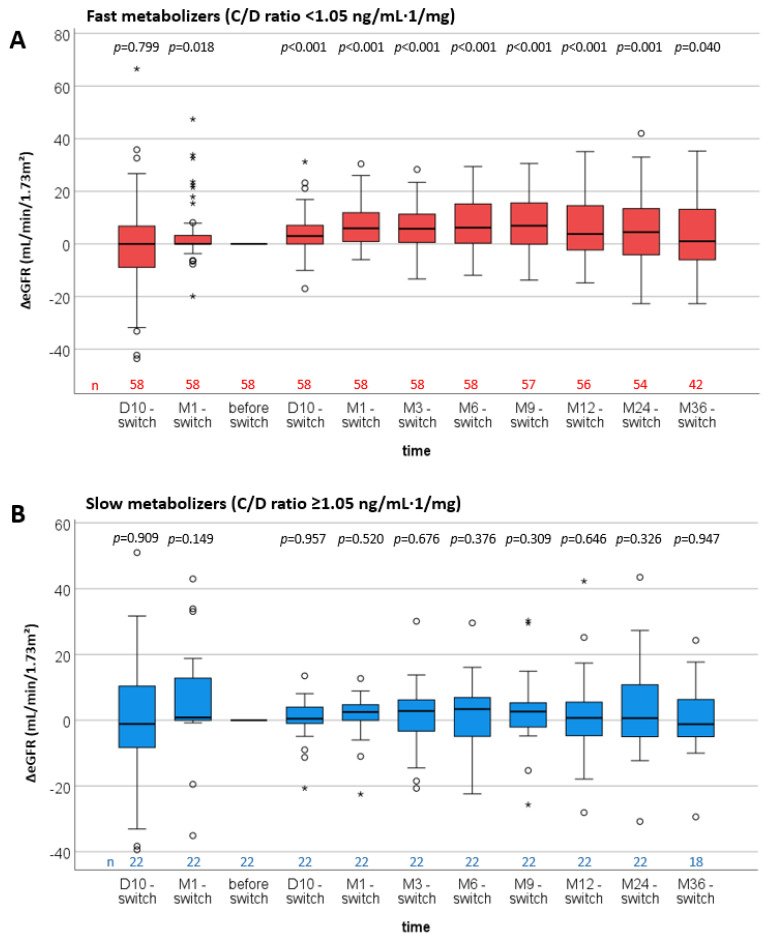
Fast tacrolimus (Tac) metabolism is associated with a more rapid decline of renal function after renal transplantation (RTx). Because the pharmacokinetics of LCP-Tac (LCPT) and immediate-release Tac (IR-Tac) differ, we hypothesized that switching from IR-Tac to LCPT in kidney transplant recipients would improve the estimated glomerular filtration rate (eGFR), particularly in fast metabolizers. For proof of concept, we performed a pilot study including RTx patients who received de novo immunosuppression with IR-Tac. A Tac concentration-to-dose ratio (C/D ratio) < 1.05 ng/mL·1/mg defined fast metabolizers and ≥1.05 ng/mL·1/mg slow metabolizers one month after RTx. Patients were switched to LCPT ≥ 1 month after transplantation and followed for 3 years. Fast metabolizers (n = 58) were switched to LCPT earlier than slow metabolizers (n = 22) after RTx (2.0 (1.0−253.1) vs. 13.2 (1.2−172.8) months, p = 0.005). Twelve months after the conversion to LCPT, Tac doses were reduced by about 65% in both groups. The C/D ratios at 12 months had increased from 0.66 (0.24−2.10) to 1.74 (0.42−5.43) in fast and from 1.15 (0.32−3.60) to 2.75 (1.08−5.90) in slow metabolizers. Fast metabolizers showed noticeable recovery of mean eGFR already one month after the conversion (48.5 ± 17.6 vs. 41.5 ± 17.0 mL/min/1.73 m², p = 0.032) and at all subsequent time points, whereas the eGFR in slow metabolizers remained stable. Switching to LCPT increased Tac bioavailability, C/D ratio, and was associated with a noticeable recovery of renal function in fast metabolizers. Conversion to LCPT is safe and beneficial early after RTx.
他克莫司(Tac)代谢快与肾移植(RTx)后肾功能更快下降相关。由于长效他克莫司(LCP-Tac)和速释他克莫司(IR-Tac)的药代动力学不同,我们推测肾移植受者从IR-Tac转换为LCPT会改善估计肾小球滤过率(eGFR),尤其是在快代谢者中。为了验证这一概念,我们进行了一项试点研究,纳入接受IR-Tac初始免疫抑制的RTx患者。RTx后1个月时,他克莫司浓度与剂量比(C/D比)<1.05 ng/mL·1/mg定义为快代谢者,≥1.05 ng/mL·1/mg定义为慢代谢者。患者在移植后≥1个月转换为LCPT并随访3年。RTx后,快代谢者(n = 58)比慢代谢者(n = 22)更早转换为LCPT(2.0(1.0 - 253.1)个月对13.2(1.2 - 172.8)个月,p = 0.005)。转换为LCPT后12个月,两组的他克莫司剂量均降低了约65%。快代谢者12个月时的C/D比从0.66(0.24 - 2.10)增加到1.74(0.42 - 5.43),慢代谢者从1.15(0.32 - 3.60)增加到2.75(1.08 - 5.90)。快代谢者在转换后1个月时平均eGFR就已显著恢复(48.5±17.6对41.5±17.0 mL/min/1.73 m²,p = 0.032),且在所有后续时间点均如此,而慢代谢者的eGFR保持稳定。转换为LCPT可提高他克莫司的生物利用度、C/D比,并与快代谢者肾功能的显著恢复相关。肾移植后早期转换为LCPT是安全且有益的。