Department of Cardiology Aarhus University Hospital Aarhus Denmark.
Department of Internal Medicine Horsens Regional Hospital Horsens Denmark.
J Am Heart Assoc. 2020 Feb 4;9(3):e014795. doi: 10.1161/JAHA.119.014795. Epub 2020 Jan 25.
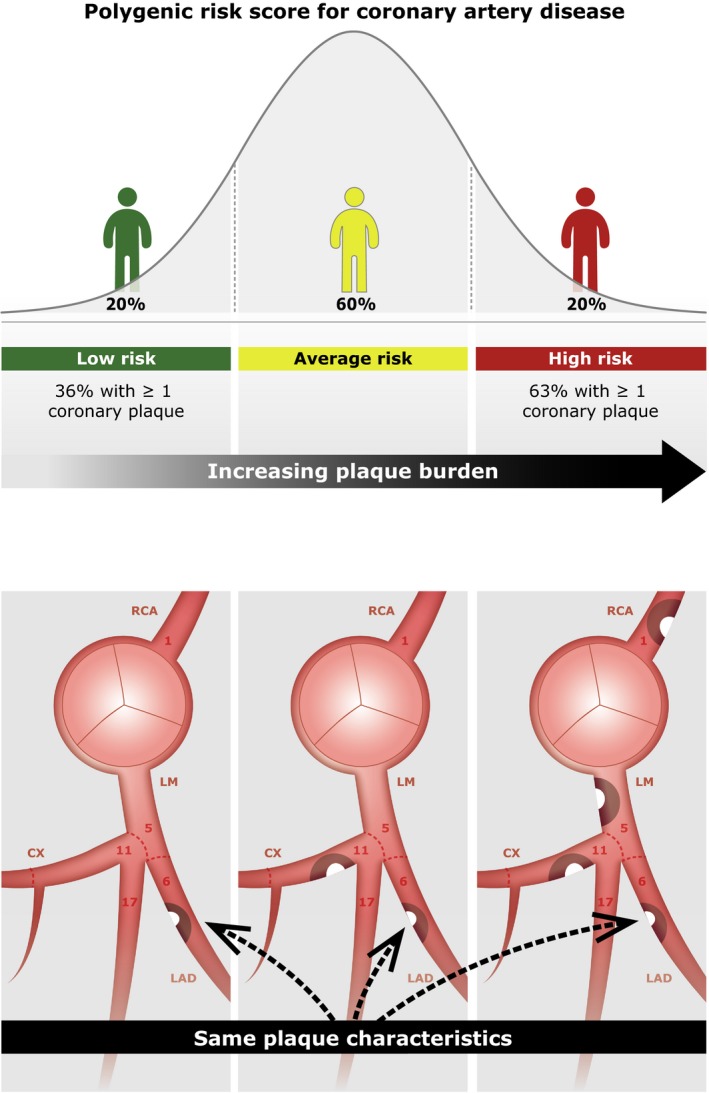
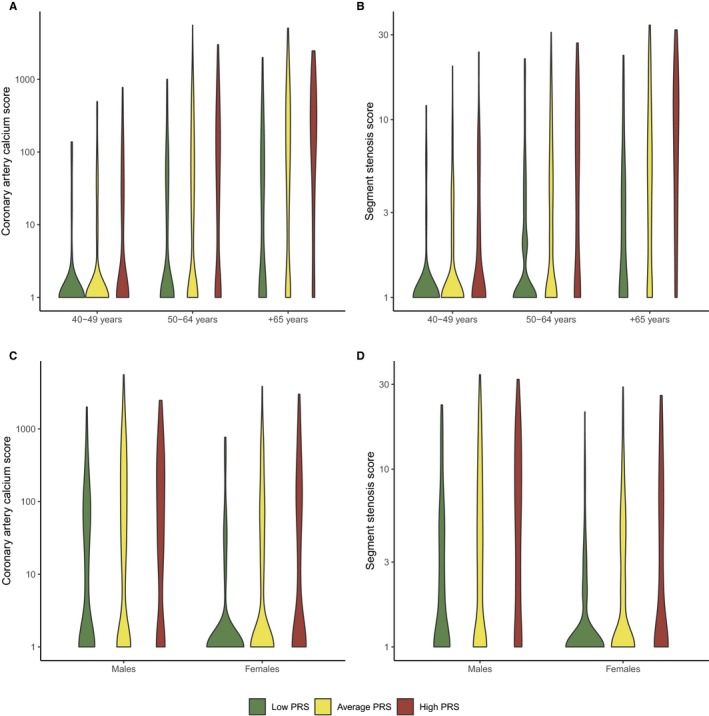
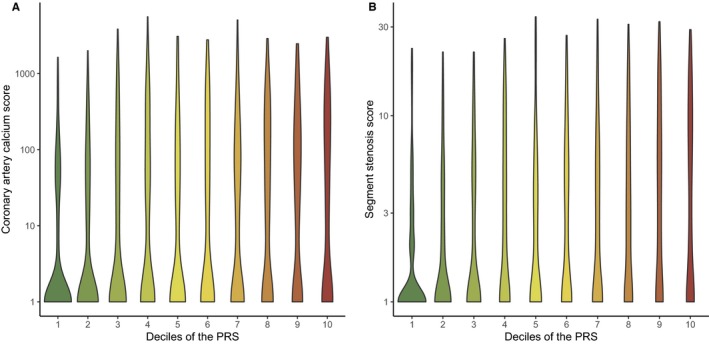
Background Polygenic risk scores (PRSs) based on risk variants from genome-wide association studies predict coronary artery disease (CAD) risk. However, it is unknown whether the PRS is associated with specific CAD characteristics. Methods and Results We consecutively included 1645 patients with suspected stable CAD undergoing coronary computed tomography angiography. A multilocus PRS was calculated as the weighted sum of CAD risk variants. Plaques were evaluated using an 18-segment model and characterized by stenosis severity and composition (soft [0%-19% calcified], mixed-soft [20%-49% calcified], mixed-calcified [50%-79% calcified], or calcified [≥80% calcified]). Coronary artery calcium score and segment stenosis score were used to characterize plaque burden. For each standard deviation increase in the PRS, coronary artery calcium score increased by 78% (=4.1e-26) and segment stenosis score increased by 16% (=2.4e-29) in the fully adjusted model. The PRS was associated with a higher prevalence of obstructive plaques (odds ratio [OR: 1.78, =5.6e-16), calcified (OR: 1.69, =6.5e-17), mixed-calcified (OR: 1.67, =7.3e-9), mixed-soft (OR: 1.45, =1.6e-6), and soft plaques (OR: 1.49, =2.5e-6), and a higher prevalence of plaque in each coronary vessel (all <1.0e-4). However, when analyzing data on a plaque level (3007 segments with plaque in 849 patients) the PRS was not associated with stenosis severity, plaque composition, or localization (all >0.05). Conclusions Our results suggest that polygenic risk based on large genome-wide association studies increases CAD risk through an increased burden of coronary atherosclerosis rather than promoting specific plaque features. Clinical Trial Registration URL: https://www.clinicaltrials.gov. Unique identifier: NCT02264717.
基于全基因组关联研究中风险变异的多基因风险评分(PRSs)可预测冠心病(CAD)风险。然而,尚不清楚 PRS 是否与特定 CAD 特征相关。
我们连续纳入了 1645 例疑似稳定型 CAD 行冠状动脉计算机断层扫描血管造影的患者。多基因 PRS 作为 CAD 风险变异的加权和计算。使用 18 节段模型评估斑块,并通过狭窄严重程度和组成(软斑块[0%-19%钙化]、混合软斑块[20%-49%钙化]、混合钙化斑块[50%-79%钙化]或钙化斑块[≥80%钙化])进行特征描述。冠状动脉钙评分和节段狭窄评分用于评估斑块负担。在完全调整模型中,PRS 每增加一个标准差,冠状动脉钙评分增加 78%(=4.1e-26),节段狭窄评分增加 16%(=2.4e-29)。PRS 与更高比例的阻塞性斑块(比值比[OR]:1.78,=5.6e-16)、钙化斑块(OR:1.69,=6.5e-17)、混合钙化斑块(OR:1.67,=7.3e-9)、混合软斑块(OR:1.45,=1.6e-6)和软斑块(OR:1.49,=2.5e-6)相关,且每支冠状动脉的斑块发生率均较高(均<1.0e-4)。然而,当在斑块水平上进行数据分析(849 例患者中有 3007 个斑块节段)时,PRS 与狭窄严重程度、斑块成分或定位均无相关性(均>0.05)。
我们的结果表明,基于大型全基因组关联研究的多基因风险通过增加冠状动脉粥样硬化负担而不是促进特定斑块特征来增加 CAD 风险。
https://www.clinicaltrials.gov。
NCT02264717。