Department of Pharmacology and Molecular Sciences, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
Center for Tuberculosis Research, Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
J Infect Dis. 2021 Jun 4;223(11):1855-1864. doi: 10.1093/infdis/jiaa016.
Linezolid (LZD) is bactericidal against Mycobacterium tuberculosis, but it has treatment-limiting toxicities. A better understanding of exposure-response relationships governing LZD efficacy and toxicity will inform dosing strategies. Because in vitro monotherapy studies yielded conflicting results, we explored LZD pharmacokinetic/pharmacodynamic (PK/PD) relationships in vivo against actively and nonactively multiplying bacteria, including in combination with pretomanid.
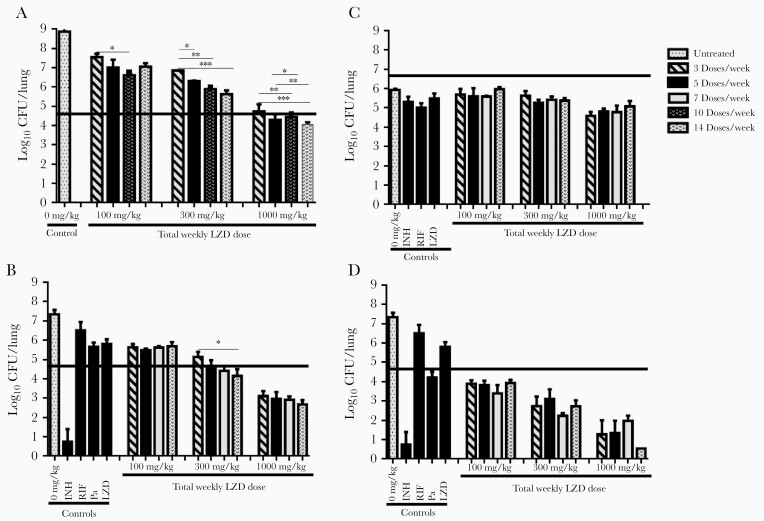
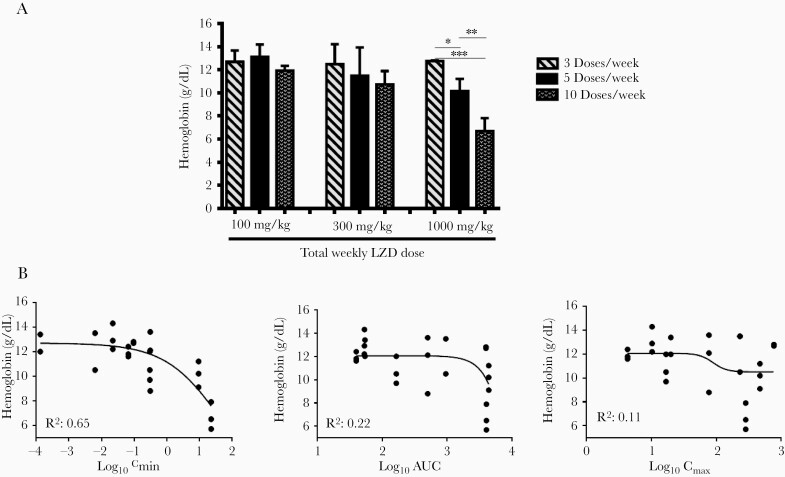
Linezolid multidose pharmacokinetics were modeled in mice. Dose-fractionation studies were performed in acute (net bacterial growth) and chronic (no net growth) infection models. In acute models, LZD was administered alone or with bacteriostatic or bactericidal pretomanid doses. Correlations between PK/PD parameters and lung colony-forming units (CFUs) and complete blood counts were assessed.
Overall, time above minimum inhibitory concentration (T>MIC) correlated best with CFU decline. However, in growth-constrained models (ie, chronic infection, coadministration with pretomanid 50 mg/kg per day), area under the concentration-time curve over MIC (AUC/MIC) had similar explanatory power. Red blood cell counts correlated strongly with LZD minimum concentration (Cmin).
Although T>MIC was the most consistent correlate of efficacy, AUC/MIC was equally predictive when bacterial multiplication was constrained by host immunity or pretomanid. In effective combination regimens, administering the same total LZD dose less frequently may be equally effective and cause less Cmin-dependent toxicity.
利奈唑胺(LZD)对结核分枝杆菌具有杀菌作用,但具有治疗限制毒性。更好地了解控制 LZD 疗效和毒性的暴露-反应关系将为剂量策略提供信息。由于体外单药治疗研究得出了相互矛盾的结果,我们在体内探索了 LZD 药代动力学/药效学(PK/PD)与主动和非增殖细菌的关系,包括与普托马尼德联合治疗。
在小鼠中对利奈唑胺进行了多剂量药代动力学建模。在急性(细菌净生长)和慢性(无净生长)感染模型中进行了剂量分割研究。在急性模型中,单独或与抑菌或杀菌剂量的普托马尼德联合给药。评估了 PK/PD 参数与肺菌落形成单位(CFU)和全血细胞计数之间的相关性。
总体而言,高于最小抑菌浓度(T>MIC)的时间与 CFU 下降相关性最好。然而,在生长受限模型(即慢性感染,与普托马尼德 50mg/kg/天联合给药)中,MIC 下浓度-时间曲线下面积(AUC/MIC)具有相似的解释能力。红细胞计数与 LZD 最小浓度(Cmin)密切相关。
尽管 T>MIC 是最一致的疗效相关性指标,但在宿主免疫或普托马尼德受到限制时,AUC/MIC 也具有同等的预测性。在有效的联合治疗方案中,以较低的频率给予相同的总 LZD 剂量可能同样有效,并且引起的 Cmin 依赖性毒性较小。