Centre for Midwifery and Child and Family Health, Faculty of Health, University of Technology Sydney, Australia.
Department of Medicine, Western Sydney University, Sydney, Australia.
PLoS One. 2020 Jan 29;15(1):e0228196. doi: 10.1371/journal.pone.0228196. eCollection 2020.
The proportion of women undergoing induction of labour (IOL) has risen in recent decades, with significant variation within countries and between hospitals. The aim of this study was to review research supporting indications for IOL and determine which indications are supported by evidence and where knowledge gaps exist.
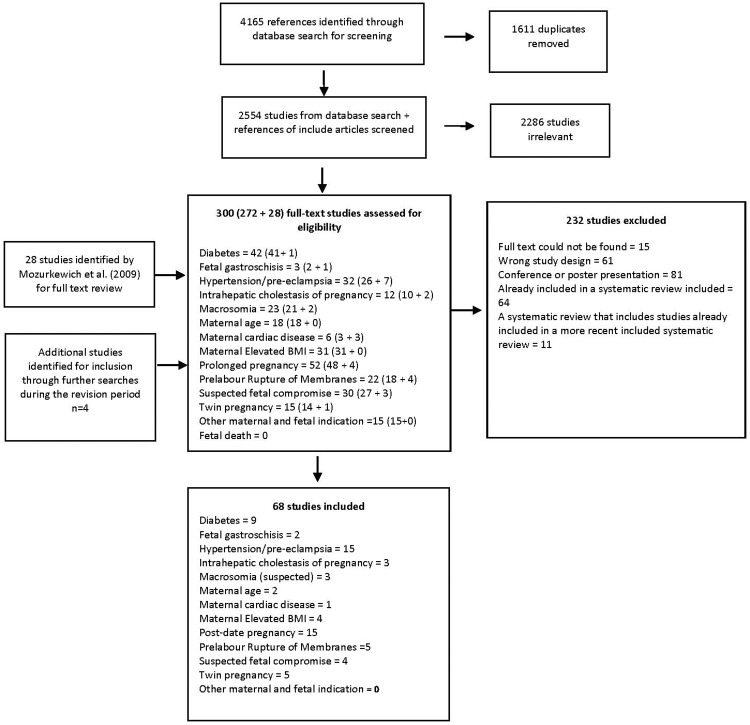
A systematic scoping review of quantitative studies of common indications for IOL. For each indication, we included systematic reviews/meta-analyses, randomised controlled trials (RCTs), cohort studies and case control studies that compared maternal and neonatal outcomes for different modes or timing of birth. Studies were identified via the databases PubMed, Maternity and Infant Care, CINAHL, EMBASE, and ClinicalTrials.gov from between April 2008 and November 2019, and also from reference lists of included studies. We identified 2554 abstracts and reviewed 300 full text articles. The quality of included studies was assessed using the RoB 2.0, the ROBINS-I and the ROBIN tool.
68 studies were included which related to post-term pregnancy (15), hypertension/pre-eclampsia (15), diabetes (9), prelabour rupture of membranes (5), twin pregnancy (5), suspected fetal compromise (4), maternal elevated body mass index (BMI) (4), intrahepatic cholestasis of pregnancy (3), suspected macrosomia (3), fetal gastroschisis (2), maternal age (2), and maternal cardiac disease (1). Available evidence supports IOL for women with post-term pregnancy, although the evidence is weak regarding the timing (41 versus 42 weeks), and for women with hypertension/preeclampsia in terms of improved maternal outcomes. For women with preterm premature rupture of membranes (24-37 weeks), high-quality evidence supports expectant management rather than IOL/early birth. Evidence is weakly supportive for IOL in women with term rupture of membranes. For all other indications, there were conflicting findings and/or insufficient power to provide definitive evidence.
While for some indications, IOL is clearly recommended, a number of common indications for IOL do not have strong supporting evidence. Overall, few RCTs have evaluated the various indications for IOL. For conditions where clinical equipoise regarding timing of birth may still exist, such as suspected macrosomia and elevated BMI, researchers and funding agencies should prioritise studies of sufficient power that can provide quality evidence to guide care in these situations.
近年来,接受引产(IOL)的女性比例有所上升,在国家内部和医院之间存在显著差异。本研究旨在回顾支持 IOL 适应证的研究,并确定哪些适应证有证据支持,哪些适应证存在知识空白。
对常见 IOL 适应证的定量研究进行系统范围的综述。对于每一个适应证,我们纳入了比较不同分娩方式或时机的母婴结局的系统评价/荟萃分析、随机对照试验(RCT)、队列研究和病例对照研究。研究通过数据库 PubMed、Maternity and Infant Care、CINAHL、EMBASE 和 ClinicalTrials.gov 于 2008 年 4 月至 2019 年 11 月间进行检索,并对纳入研究的参考文献进行了补充检索。我们共检索到 2554 篇摘要,并对 300 篇全文文章进行了评审。使用 RoB 2.0、ROBINS-I 和 ROBIN 工具对纳入研究的质量进行评估。
共纳入 68 项研究,涉及过期妊娠(15 项)、高血压/子痫前期(15 项)、糖尿病(9 项)、胎膜早破(5 项)、双胎妊娠(5 项)、胎儿窘迫(4 项)、产妇超重/肥胖(4 项)、妊娠肝内胆汁淤积症(3 项)、怀疑巨大儿(3 项)、胎儿腹裂(2 项)、产妇年龄(2 项)和产妇心脏疾病(1 项)。现有证据支持对过期妊娠和高血压/子痫前期的孕妇进行 IOL,但在分娩时机(41 周与 42 周)方面证据较弱,对于胎膜早破的孕妇,期待治疗优于 IOL/早产。对于 24-37 周的早产胎膜早破孕妇,有高质量证据支持期待治疗而非 IOL/早产。对于足月胎膜早破的孕妇,IOL 有一定的支持证据。对于其他适应证,存在相互矛盾的结果和/或缺乏提供明确证据的能力。
虽然对于一些适应证,IOL 显然是推荐的,但对于一些常见的 IOL 适应证,没有强有力的支持证据。总体而言,很少有 RCT 评估了 IOL 的各种适应证。对于在分娩时机方面可能仍然存在临床争议的情况,如怀疑巨大儿和超重/肥胖,研究人员和资助机构应优先开展具有足够效能的研究,为这些情况下的治疗提供高质量的证据。