School of Mathematics, Statistics and Computer Science, University of KwaZulu-Natal, Durban, South Africa.
Department of Statistics, Durban University of Technology, Durban, South Africa.
BMC Public Health. 2020 Jan 29;20(1):126. doi: 10.1186/s12889-020-8189-8.
The causes of childhood anaemia are multifactorial, interrelated and complex. Such causes vary from country to country, and within a country. Thus, strategies for anaemia control should be tailored to local conditions and take into account the specific etiology and prevalence of anaemia in a given setting and sub-population. In addition, policies and programmes for anaemia control that do not account for the spatial heterogeneity of anaemia in children may result in certain sub-populations being excluded, limiting the effectiveness of the programmes. This study investigated the demographic and socio-economic determinants as well as the spatial variation of anaemia in children aged 6 to 59 months in Kenya, Malawi, Tanzania and Uganda.
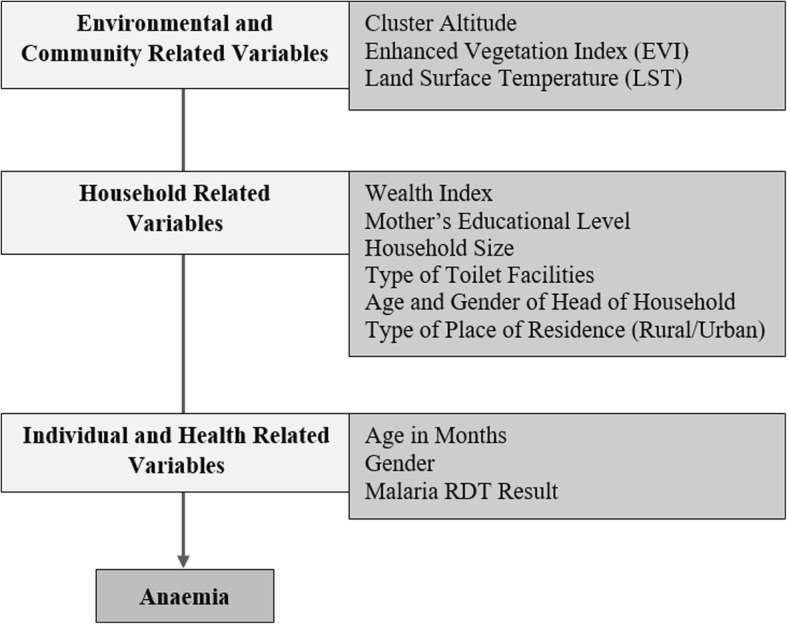
The study made use of data collected from nationally representative Malaria Indicator Surveys (MIS) and Demographic and Health Surveys (DHS) conducted in all four countries between 2015 and 2017. During these surveys, all children under the age of five years old in the sampled households were tested for malaria and anaemia. A child's anaemia status was based on the World Health Organization's cut-off points where a child was considered anaemic if their altitude adjusted haemoglobin (Hb) level was less than 11 g/dL. The explanatory variables considered comprised of individual, household and cluster level factors, including the child's malaria status. A multivariable hierarchical Bayesian geoadditive model was used which included a spatial effect for district of child's residence.
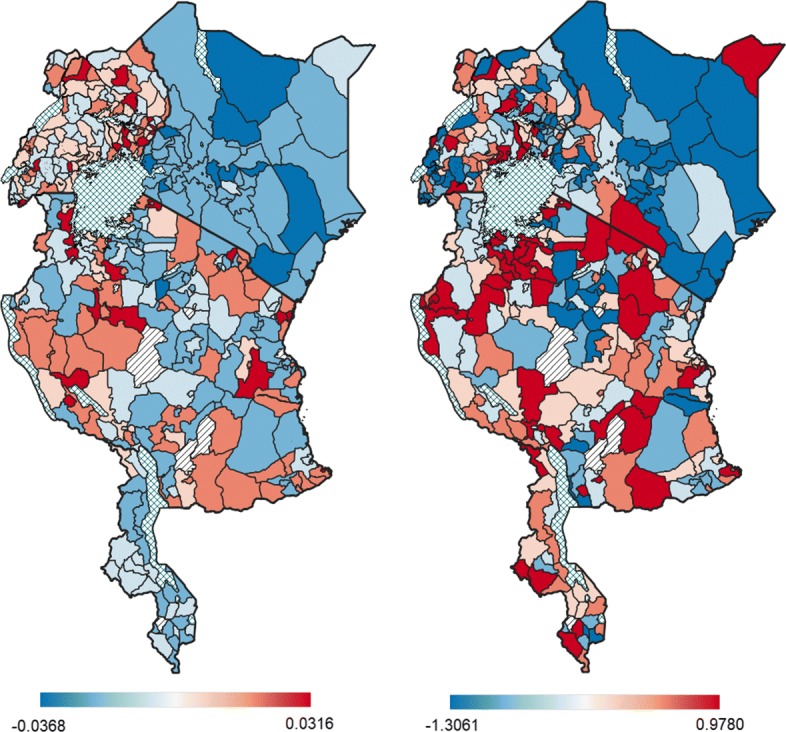
Prevalence of childhood anaemia ranged from 36.4% to 61.9% across the four countries. Children with a positive malaria result had a significantly higher odds of anaemia [AOR = 4.401; 95% CrI: (3.979, 4.871)]. After adjusting for a child's malaria status and other demographic, socio-economic and environmental factors, the study revealed distinct spatial variation in childhood anaemia within and between Malawi, Uganda and Tanzania. The spatial variation appeared predominantly due to unmeasured district-specific factors that do not transcend boundaries.
Anaemia control measures in Malawi, Tanzania and Uganda need to account for internal spatial heterogeneity evident in these countries. Efforts in assessing the local district-specific causes of childhood anaemia within each country should be focused on.
儿童贫血的原因是多因素的、相互关联的和复杂的。这些原因因国家而异,在一个国家内也是如此。因此,贫血控制策略应因地制宜,并考虑到特定环境和亚人群中贫血的具体病因和流行率。此外,不考虑儿童贫血的空间异质性的贫血控制政策和方案可能导致某些亚人群被排除在外,从而限制了方案的有效性。本研究调查了肯尼亚、马拉维、坦桑尼亚和乌干达 6 至 59 个月儿童贫血的人口统计学和社会经济决定因素以及空间变化。
本研究利用了 2015 年至 2017 年在所有四个国家进行的全国代表性疟疾指标调查(MIS)和人口与健康调查(DHS)收集的数据。在这些调查中,抽样家庭中所有五岁以下的儿童都接受了疟疾和贫血检测。儿童的贫血状况基于世界卫生组织的截止值,如果儿童的海拔调整血红蛋白(Hb)水平低于 11g/dL,则认为该儿童贫血。考虑的解释变量包括个人、家庭和群体层面的因素,包括儿童的疟疾状况。使用多变量分层贝叶斯地理加法模型,其中包括儿童居住地的区的空间效应。
四个国家的儿童贫血患病率从 36.4%到 61.9%不等。患有阳性疟疾结果的儿童贫血的可能性显著更高[优势比(AOR)=4.401;95%可信区间(CrI):(3.979,4.871)]。在调整了儿童的疟疾状况以及其他人口统计学、社会经济和环境因素后,研究显示了马拉维、乌干达和坦桑尼亚境内和之间儿童贫血的明显空间差异。空间差异主要是由于无法跨越边界的未测量的特定地区因素造成的。
马拉维、坦桑尼亚和乌干达的贫血控制措施需要考虑到这些国家内存在的内部空间异质性。应集中精力评估每个国家内当地特定地区导致儿童贫血的原因。