Department of Internal Medicine and Cardiology, Charité - Universitätsmedizin Berlin, Campus Virchow Klinikum, Medizinische Klinik m. S. Kardiologie, Augustenburger Platz 1, 13353, Berlin, Germany.
DZHK (German Centre for Cardiovascular Research), partner site Berlin, Berlin, Germany.
ESC Heart Fail. 2020 Jun;7(3):942-952. doi: 10.1002/ehf2.12605. Epub 2020 Jan 30.
Whereas syncopal episodes are a frequent complication of cardiovascular disorders, including heart failure (HF), little is known whether syncopes impact the prognosis of patients with HF. We aimed to assess the impact of a history of syncope (HoS) on overall and hospitalization-free survival of these patients.
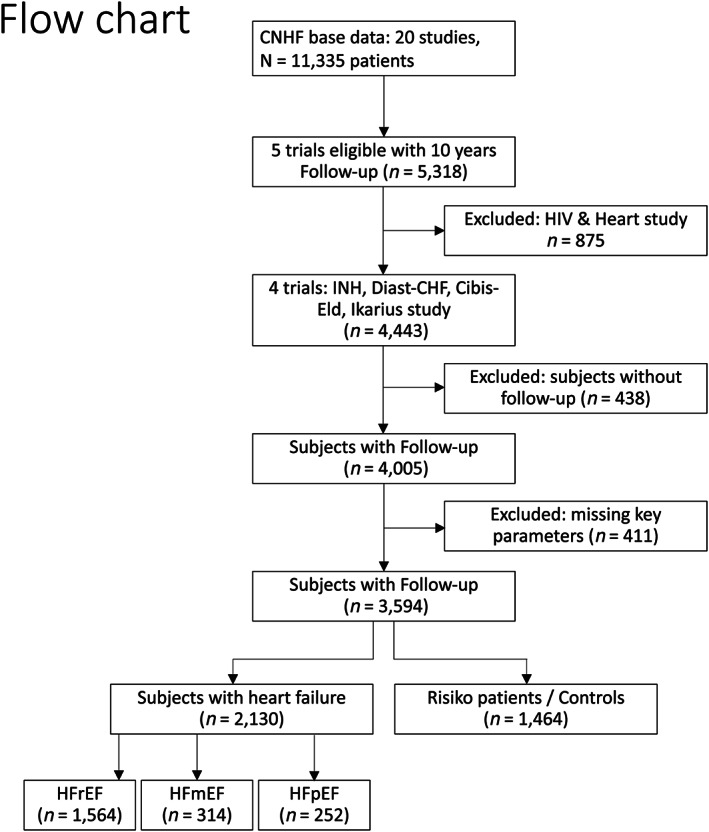
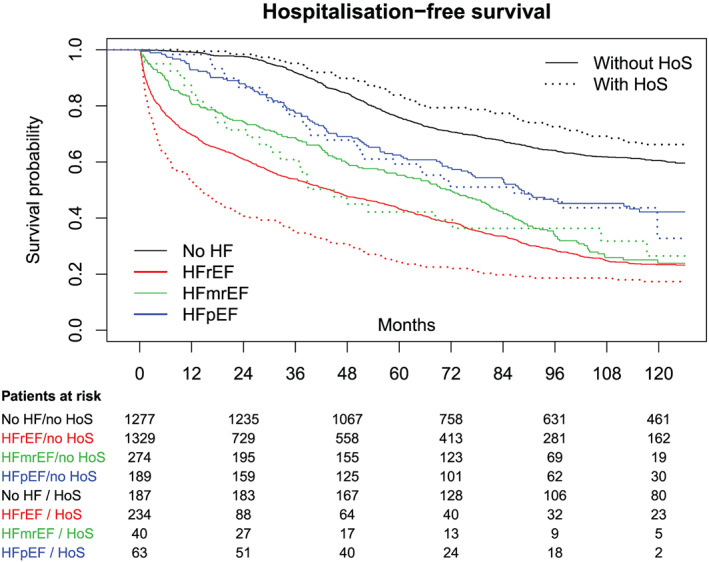
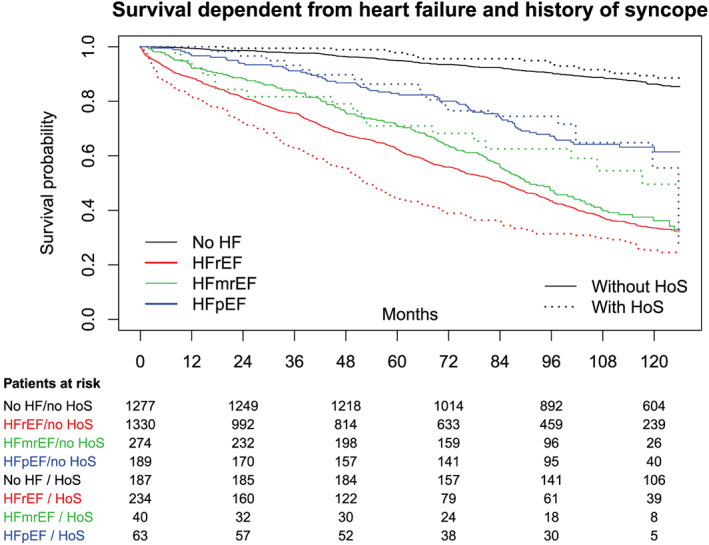
We pooled the data of prospective, nationwide, multicentre studies conducted within the framework of the German Competence Network for Heart Failure including 11 335 subjects. Excluding studies with follow-up periods <10 years, we assessed 5318 subjects. We excluded a study focusing on cardiac changes in patients with an HIV infection because of possible confounding factors and 849 patients due to either missing key parameters or missing follow-up data, resulting in 3594 eligible subjects, including 2130 patients with HF [1564 patients with heart failure with reduced ejection fraction (HFrEF), 314 patients with heart failure with mid-range ejection fraction, and 252 patients with heart failure with preserved ejection fraction (HFpEF)] and 1464 subjects without HF considered as controls. HoS was more frequent in the overall cohort of patients with HF compared with controls (P < 0.001)-mainly driven by the HFpEF subgroup (HFpEF vs. controls: 25.0% vs. 12.8%, P < 0.001). Of all the subjects, 14.6% reported a HoS. Patients with HFrEF in our pooled cohort showed more often syncopes than subjects without HF (15.0% vs. 12.8%, P = 0.082). Subjects with HoS showed worse overall survival [42.4% vs. 37.9%, hazard ratio (HR) = 1.21, 99% confidence interval (0.99, 1.46), P = 0.04] and less days alive out of hospital [HR = 1.39, 99% confidence interval (1.18, 1.64), P < 0.001] compared with all subjects without HoS. Patients with HFrEF with HoS died earlier [30.3% vs. 41.6%, HR = 1.40, 99% confidence interval (1.12, 1.74), P < 0.001] and lived fewer days out of hospital than those without HoS. We could not find these changes in mortality and hospital-free survival in the heart failure with mid-range ejection fraction and HFpEF cohorts. HoS represented a clinically high-risk profile within the HFrEF group-combining different risk factors. Further analyses showed that among patients with HFrEF with HoS, known cardiovascular risk factors (e.g. age, male sex, diabetes mellitus, and anaemia) were more prevalent. These constellations of the risk factors explained the effect of HoS in a multivariable Cox regression models.
In a large cohort of patients with HF, HoS was found to be a clinically and easily accessible predictor of both overall and hospitalization-free survival in patients with HFrEF and should thus routinely be assessed.
晕厥发作是心血管疾病(包括心力衰竭[HF])的常见并发症,但晕厥是否影响 HF 患者的预后知之甚少。我们旨在评估晕厥史(HoS)对这些患者总生存率和无住院生存率的影响。
我们汇总了在德国心力衰竭协作网络框架内进行的前瞻性、全国性、多中心研究的数据,其中包括 11335 例患者。排除随访期<10 年的研究后,我们评估了 5318 例患者。我们排除了一项专门研究 HIV 感染患者心脏变化的研究,因为可能存在混杂因素,此外还排除了 849 例因关键参数缺失或随访数据缺失的患者,最终纳入 3594 例合格患者,其中 2130 例 HF 患者[射血分数降低的心力衰竭(HFrEF)患者 1564 例、射血分数中间范围的心力衰竭患者 314 例、射血分数保留的心力衰竭(HFpEF)患者 252 例]和 1464 例无 HF 的患者作为对照。与对照组相比,HF 患者总体队列中 HoS 更为常见(P<0.001)-主要是由 HFpEF 亚组驱动的(HFpEF 与对照组:25.0%与 12.8%,P<0.001)。在所有患者中,有 14.6%报告了 HoS。我们汇总队列中的 HFrEF 患者比无 HF 的患者更常发生晕厥(15.0%与 12.8%,P=0.082)。有 HoS 的患者总生存率较差[42.4%与 37.9%,风险比(HR)=1.21,99%置信区间(0.99,1.46),P=0.04],无住院天数较少[HR=1.39,99%置信区间(1.18,1.64),P<0.001]与所有无 HoS 的患者相比。有 HoS 的 HFrEF 患者更早死亡[30.3%与 41.6%,HR=1.40,99%置信区间(1.12,1.74),P<0.001],无住院天数较少。我们在射血分数中间范围和 HFpEF 队列中没有发现死亡率和无住院生存率的这些变化。HoS 在 HFrEF 组中代表了一种临床高风险特征-合并了不同的危险因素。进一步分析显示,在有 HoS 的 HFrEF 患者中,已知心血管危险因素(如年龄、男性、糖尿病和贫血)更为普遍。这些危险因素的组合在多变量 Cox 回归模型中解释了 HoS 的作用。
在 HF 患者的大型队列中,发现 HoS 是 HFrEF 患者总生存率和无住院生存率的临床和易于获得的预测因素,因此应常规评估。