Takagi Yusuke, Osawa Gakuji, Kato Yoriko, Ikezawa Eri, Kobayashi Chika, Aruga Etsuko
Department of Palliative Medicine, Teikyo University School of Medicine, 2-11-1 Kaga, Itabashi-ku, Tokyo, 173-8605, Japan.
Toda-chuo General Hospital, 1-19-3 Honcho, Toda City, Saitama, 335-0023, Japan.
BMC Gastroenterol. 2020 Jan 31;20(1):25. doi: 10.1186/s12876-020-1173-z.
Naldemedine, a novel peripherally-acting mu-opioid receptor antagonist, has improved opioid-induced constipation in randomized controlled trials. The most frequent adverse event of naldemedine is diarrhea, which can cause abdominal pain and often leads to treatment discontinuation. We aimed to identify risk factors and appropriate management strategies for key adverse events including diarrhea associated with naldemedine, since those have not been extensively studied.
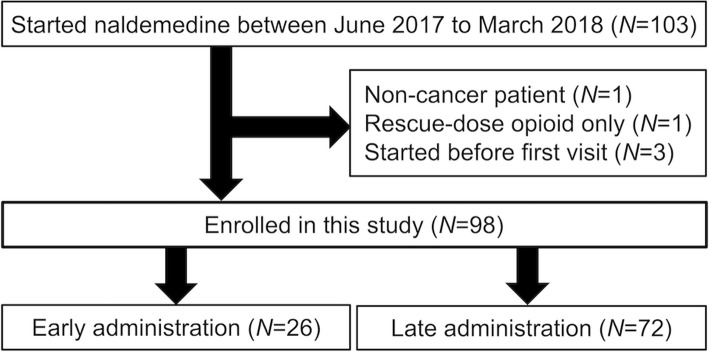
We conducted a multi-center retrospective cohort study. Eligible patients had cancer, had undergone palliative care at participating centers, had been prescribed regular opioids, and had taken at least one dose of naldemedine between June 2017 and March 2018. The primary endpoint was the incidence of diarrhea according to baseline characteristics. Secondary endpoints included the duration of naldemedine administration, daily defecation counts before and after starting naldemedine, duration and severity of diarrhea as an adverse event of naldemedine, other adverse events, and the incidence of constipation within 7 days after recovery from diarrhea. We defined patients who started naldemedine within three days of starting a regularly prescribed opioid as the early group, and the remainder as the late group.
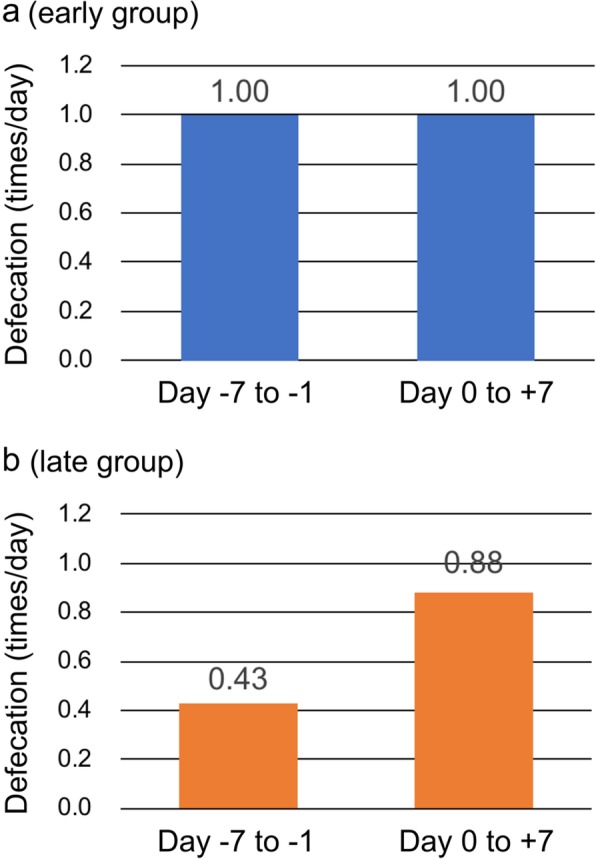
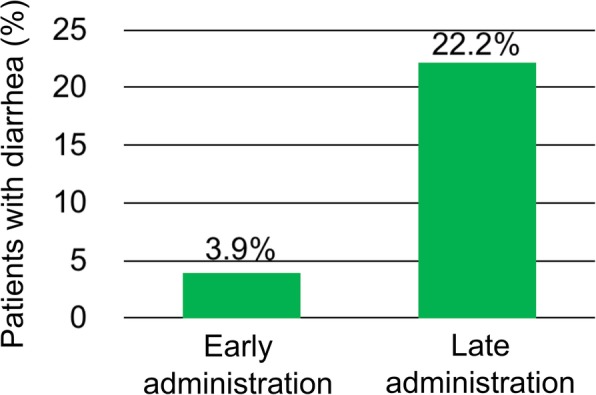
Among 103 patients who received naldemedine, 98 fulfilled the eligibility criteria. The median age was 68 years and 48% of the patients were female. Median performance status was 3, and the median oral intake was 50%. The median duration of naldemedine administration and overall survival were 25 and 64 days, respectively. The incidence of diarrhea in the early group (n = 26) was significantly lower than in the late group (n = 72) (3.9% vs. 22.2%, p = 0.02). Daily defecation counts increased after late (median 0.43 to 0.88, p < 0.001), but remained stable after early naldemedine administration (median 1.00 to 1.00, p = 0.34). Constipation after the diarrhea was resolved was common (53%), especially among patients who stopped naldemedine (78%). The diarrhea was improved within three days in 92% of patients who stopped other laxatives.
The early administration of naldemedine is beneficial because it reduces adverse events including diarrhea. Diarrhea caused by naldemedine can be effectively managed by stopping other laxatives while continuing naldemedine.
纳洛酮是一种新型外周作用的μ-阿片受体拮抗剂,在随机对照试验中改善了阿片类药物引起的便秘。纳洛酮最常见的不良事件是腹泻,腹泻可引起腹痛,并常导致治疗中断。我们旨在确定包括与纳洛酮相关的腹泻在内的关键不良事件的危险因素和适当的管理策略,因为这些尚未得到广泛研究。
我们进行了一项多中心回顾性队列研究。符合条件的患者患有癌症,在参与中心接受过姑息治疗,已被处方常规阿片类药物,并且在2017年6月至2018年3月期间服用过至少一剂纳洛酮。主要终点是根据基线特征的腹泻发生率。次要终点包括纳洛酮给药持续时间、开始纳洛酮治疗前后的每日排便次数、作为纳洛酮不良事件的腹泻持续时间和严重程度、其他不良事件以及腹泻恢复后7天内便秘的发生率。我们将在开始常规处方阿片类药物后三天内开始使用纳洛酮的患者定义为早期组,其余患者定义为晚期组。
在103例接受纳洛酮治疗的患者中,98例符合纳入标准。中位年龄为68岁,48%的患者为女性。中位体能状态为3,中位口服摄入量为50%。纳洛酮给药的中位持续时间和总生存期分别为25天和64天。早期组(n = 26)的腹泻发生率显著低于晚期组(n = 72)(3.9%对22.2%,p = 0.02)。晚期纳洛酮给药后每日排便次数增加(中位数从0.43增加到0.88,p < 0.001),但早期纳洛酮给药后保持稳定(中位数从1.00到1.00,p = 0.34)。腹泻缓解后的便秘很常见(53%),尤其是在停用纳洛酮的患者中(78%)。92%停用其他泻药的患者腹泻在三天内得到改善。
早期使用纳洛酮是有益的,因为它减少了包括腹泻在内的不良事件。纳洛酮引起的腹泻可以通过在继续使用纳洛酮的同时停用其他泻药来有效管理。