Cancer Research Division, Cancer Council NSW, Sydney, NSW, Australia; School of Public Health, Sydney Medical School, University of Sydney, Sydney, NSW, Australia; Prince of Wales Clinical School, University of New South Wales, Sydney, NSW, Australia.
Center for Health Decision Science, Harvard TH Chan School of Public Health, Boston, MA, USA.
Lancet. 2020 Feb 22;395(10224):591-603. doi: 10.1016/S0140-6736(20)30157-4. Epub 2020 Jan 30.
WHO is developing a global strategy towards eliminating cervical cancer as a public health problem, which proposes an elimination threshold of four cases per 100 000 women and includes 2030 triple-intervention coverage targets for scale-up of human papillomavirus (HPV) vaccination to 90%, twice-lifetime cervical screening to 70%, and treatment of pre-invasive lesions and invasive cancer to 90%. We assessed the impact of achieving the 90-70-90 triple-intervention targets on cervical cancer mortality and deaths averted over the next century. We also assessed the potential for the elimination initiative to support target 3.4 of the UN Sustainable Development Goals (SDGs)-a one-third reduction in premature mortality from non-communicable diseases by 2030.
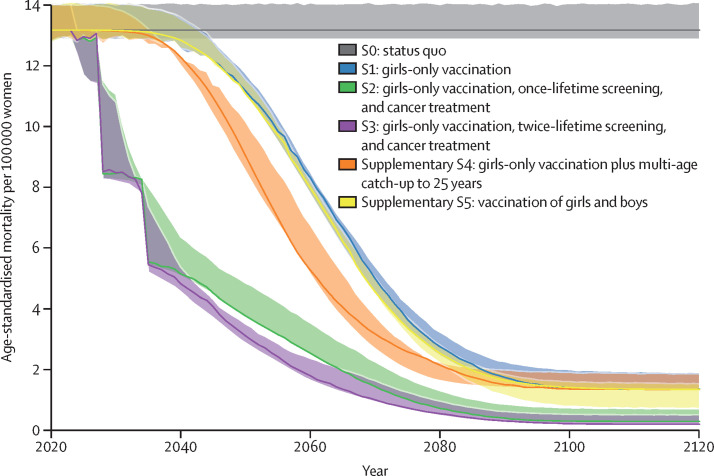
The WHO Cervical Cancer Elimination Modelling Consortium (CCEMC) involves three independent, dynamic models of HPV infection, cervical carcinogenesis, screening, and precancer and invasive cancer treatment. Reductions in age-standardised rates of cervical cancer mortality in 78 low-income and lower-middle-income countries (LMICs) were estimated for three core scenarios: girls-only vaccination at age 9 years with catch-up for girls aged 10-14 years; girls-only vaccination plus once-lifetime screening and cancer treatment scale-up; and girls-only vaccination plus twice-lifetime screening and cancer treatment scale-up. Vaccination was assumed to provide 100% lifetime protection against infections with HPV types 16, 18, 31, 33, 45, 52, and 58, and to scale up to 90% coverage in 2020. Cervical screening involved HPV testing at age 35 years, or at ages 35 years and 45 years, with scale-up to 45% coverage by 2023, 70% by 2030, and 90% by 2045, and we assumed that 50% of women with invasive cervical cancer would receive appropriate surgery, radiotherapy, and chemotherapy by 2023, which would increase to 90% by 2030. We summarised results using the median (range) of model predictions.
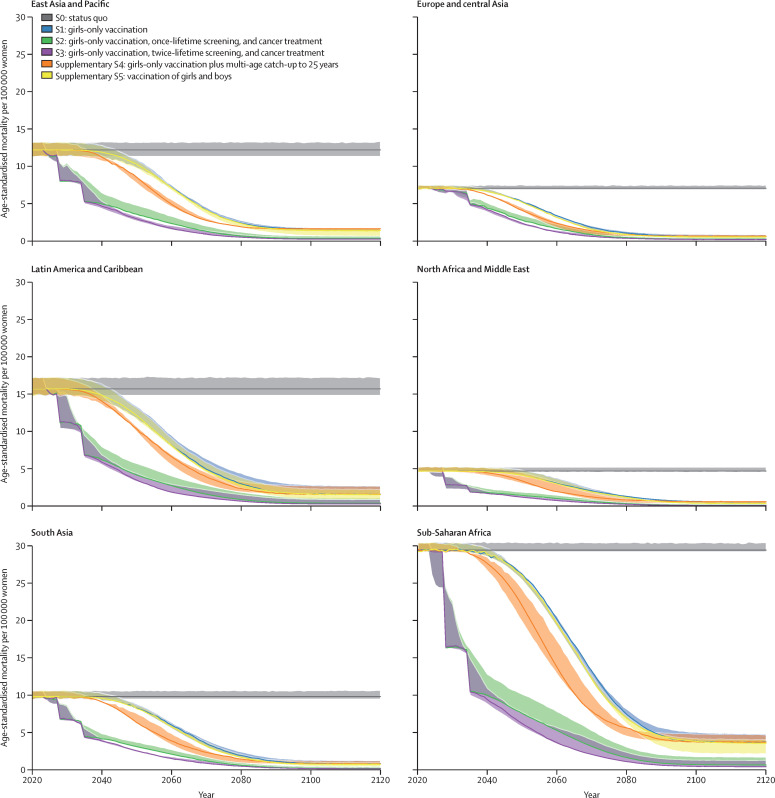
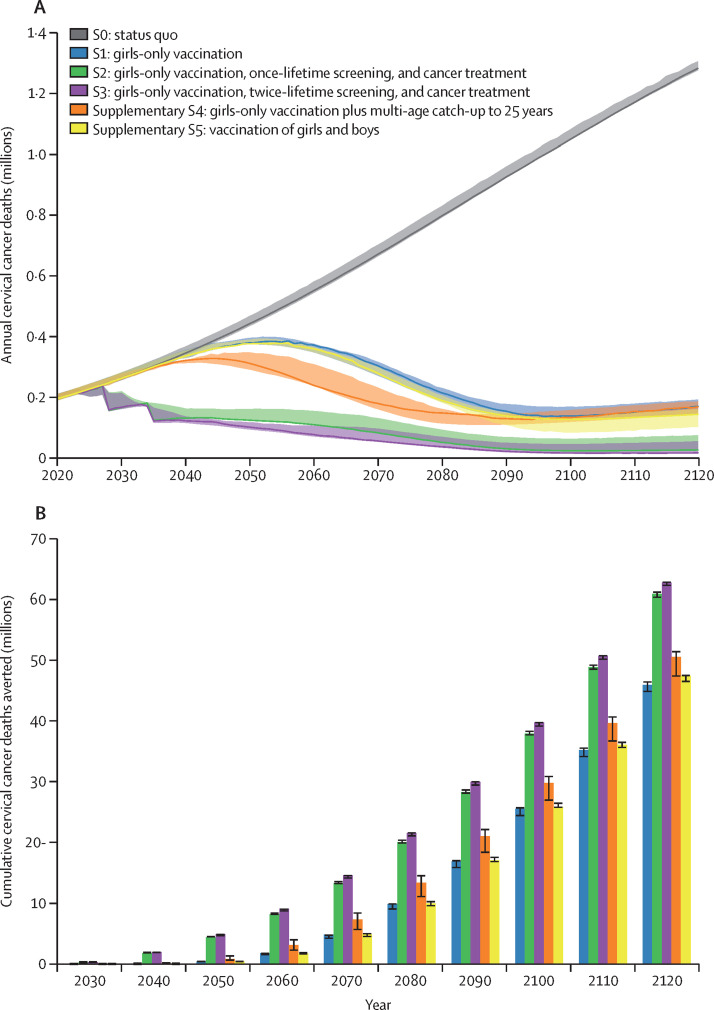
In 2020, the estimated cervical cancer mortality rate across all 78 LMICs was 13·2 (range 12·9-14·1) per 100 000 women. Compared to the status quo, by 2030, vaccination alone would have minimal impact on cervical cancer mortality, leading to a 0·1% (0·1-0·5) reduction, but additionally scaling up twice-lifetime screening and cancer treatment would reduce mortality by 34·2% (23·3-37·8), averting 300 000 (300 000-400 000) deaths by 2030 (with similar results for once-lifetime screening). By 2070, scaling up vaccination alone would reduce mortality by 61·7% (61·4-66·1), averting 4·8 million (4·1-4·8) deaths. By 2070, additionally scaling up screening and cancer treatment would reduce mortality by 88·9% (84·0-89·3), averting 13·3 million (13·1-13·6) deaths (with once-lifetime screening), or by 92·3% (88·4-93·0), averting 14·6 million (14·1-14·6) deaths (with twice-lifetime screening). By 2120, vaccination alone would reduce mortality by 89·5% (86·6-89·9), averting 45·8 million (44·7-46·4) deaths. By 2120, additionally scaling up screening and cancer treatment would reduce mortality by 97·9% (95·0-98·0), averting 60·8 million (60·2-61·2) deaths (with once-lifetime screening), or by 98·6% (96·5-98·6), averting 62·6 million (62·1-62·8) deaths (with twice-lifetime screening). With the WHO triple-intervention strategy, over the next 10 years, about half (48% [45-55]) of deaths averted would be in sub-Saharan Africa and almost a third (32% [29-34]) would be in South Asia; over the next 100 years, almost 90% of deaths averted would be in these regions. For premature deaths (age 30-69 years), the WHO triple-intervention strategy would result in rate reductions of 33·9% (24·4-37·9) by 2030, 96·2% (94·3-96·8) by 2070, and 98·6% (96·9-98·8) by 2120.
These findings emphasise the importance of acting immediately on three fronts to scale up vaccination, screening, and treatment for pre-invasive and invasive cervical cancer. In the next 10 years, a one-third reduction in the rate of premature mortality from cervical cancer in LMICs is possible, contributing to the realisation of the 2030 UN SDGs. Over the next century, successful implementation of the WHO elimination strategy would reduce cervical cancer mortality by almost 99% and save more than 62 million women's lives.
WHO, UNDP, UN Population Fund, UNICEF-WHO-World Bank Special Program of Research, Development and Research Training in Human Reproduction, Germany Federal Ministry of Health, National Health and Medical Research Council Australia, Centre for Research Excellence in Cervical Cancer Control, Canadian Institute of Health Research, Compute Canada, and Fonds de recherche du Québec-Santé.
世卫组织正在制定一项全球战略,旨在消除宫颈癌这一公共卫生问题,该战略提出消除宫颈癌的阈值为每 10 万名妇女 4 例,并包括 2030 年扩大人乳头瘤病毒(HPV)疫苗接种覆盖率至 90%、两次终生宫颈筛查覆盖率至 70%以及治疗癌前病变和浸润性癌症覆盖率至 90%的三重干预目标。我们评估了实现 90-70-90 三重干预目标对未来一个世纪宫颈癌死亡率和死亡人数的影响。我们还评估了消除倡议支持联合国可持续发展目标(SDG)目标 3.4 的潜力——到 2030 年,将非传染性疾病导致的过早死亡率降低三分之一。
世卫组织宫颈癌消除模型联盟(CCEMC)涉及三种独立的 HPV 感染、宫颈癌发生、筛查和癌前病变及浸润性癌症治疗的动态模型。估计了 78 个低收入和中低收入国家(LMICs)的宫颈癌死亡率年龄标准化率在以下三个核心情景下的降低情况:9 岁女孩接种 HPV 疫苗并为 10-14 岁女孩进行补种;HPV 疫苗接种加上一次性终生筛查和癌症治疗扩大;HPV 疫苗接种加上两次终生筛查和癌症治疗扩大。假设 HPV 疫苗接种能提供针对 HPV 16、18、31、33、45、52 和 58 型感染的 100%终身保护,并且在 2020 年覆盖率能扩大至 90%。宫颈筛查包括 35 岁时进行 HPV 检测,或在 35 岁和 45 岁时进行 HPV 检测,到 2023 年,筛查覆盖率将扩大至 45%,到 2030 年扩大至 70%,到 2045 年扩大至 90%,并且我们假设到 2023 年,50%的浸润性宫颈癌妇女将接受适当的手术、放疗和化疗,到 2030 年这一比例将增加到 90%。我们使用模型预测的中位数(范围)来总结结果。
2020 年,78 个 LMICs 的宫颈癌死亡率估计为每 10 万名妇女 13.2(范围为 12.9-14.1)。与现状相比,仅扩大 HPV 疫苗接种范围对宫颈癌死亡率的影响很小,导致死亡率降低 0.1%(0.1-0.5),但另外扩大两次终生筛查和癌症治疗将使死亡率降低 34.2%(23.3-37.8),到 2030 年将避免 30 万(30 万-40 万)人死亡(一次性终生筛查也有类似结果)。到 2070 年,仅扩大疫苗接种范围将使死亡率降低 61.7%(61.4-66.1),到 2070 年将避免 480 万(4.1-4.8)人死亡。到 2070 年,另外扩大筛查和癌症治疗将使死亡率降低 88.9%(84.0-89.3),到 2070 年将避免 1330 万(131-136)人死亡(一次性终生筛查),或 92.3%(88.4-93.0),到 2070 年将避免 1460 万(141-146)人死亡(两次终生筛查)。到 2120 年,仅扩大疫苗接种范围将使死亡率降低 89.5%(86.6-89.9),到 2120 年将避免 4580 万(447-464)人死亡。到 2120 年,另外扩大筛查和癌症治疗将使死亡率降低 97.9%(95.0-98.0),到 2120 年将避免 6080 万(602-612)人死亡(一次性终生筛查),或 98.6%(96.5-98.6),到 2120 年将避免 6260 万(621-628)人死亡(两次终生筛查)。在世卫组织三重干预战略下,未来 10 年,约一半(48%[45-55])的死亡人数将在撒哈拉以南非洲地区得到避免,近三分之一(32%[29-34])将在南亚地区得到避免;在未来 100 年,近 90%的死亡人数将在这些地区得到避免。对于 30-69 岁的过早死亡,世卫组织三重干预战略将导致 2030 年死亡率降低 33.9%(24.4-37.9),2070 年降低 96.2%(94.3-96.8),2012 年降低 98.6%(96.9-98.8)。
这些发现强调了立即采取行动扩大 HPV 疫苗接种、筛查和癌前及浸润性宫颈癌治疗的重要性。在未来 10 年,LMICs 中宫颈癌导致的过早死亡率降低三分之一是可能的,这将有助于实现 2030 年联合国可持续发展目标。在未来一个世纪,成功实施世卫组织消除战略将使宫颈癌死亡率降低近 99%,拯救超过 6200 万妇女的生命。
世卫组织、联合国开发计划署、联合国人口基金、联合国儿童基金会-世卫组织-世界银行生殖健康研究、发展和研究培训特别方案、德国联邦卫生部、澳大利亚国家卫生和医学研究理事会、宫颈癌控制卓越研究中心、加拿大卫生研究院、加拿大计算中心和魁北克省健康研究基金会。