Radiation Medicine Program, Princess Margaret Cancer Centre Toronto, Toronto, ON, Canada; Department of Radiation Oncology, University of Toronto, Toronto, ON, Canada.
Center for Health Decision Science, Harvard University, Boston, MA, USA; Department of Health Management and Health Economics, University of Oslo, Oslo, Norway.
Lancet Oncol. 2019 Jul;20(7):915-923. doi: 10.1016/S1470-2045(19)30308-0. Epub 2019 May 28.
Radiotherapy is standard of care for cervical cancer, but major global gaps in access exist, particularly in low-income and middle-income countries. We modelled the health and economic benefits of a 20-year radiotherapy scale-up to estimate the long-term demand for treatment in the context of human papillomavirus (HPV) vaccination.
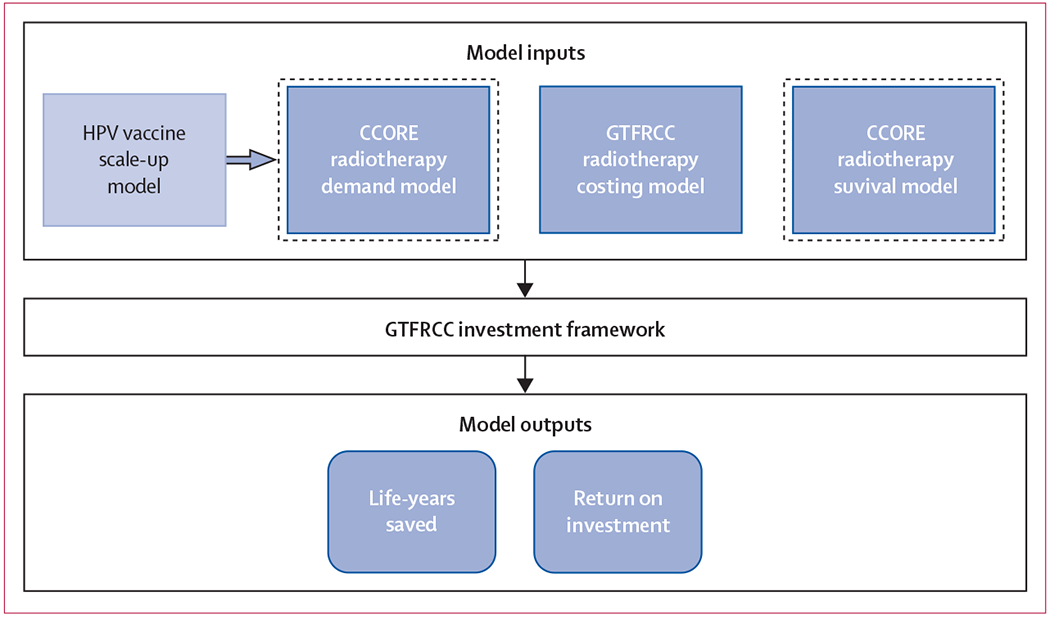
We applied the Global Task Force on Radiotherapy for Cancer Control investment framework to model the health and economic benefits of scaling up external-beam radiotherapy and brachytherapy for cervical cancer in upper-middle-income, lower-middle-income, and low-income countries between 2015 and 2035. We estimated the unique costs of external-beam radiotherapy and brachytherapy and included a specific valuation of women's caregiving contributions. Model outcomes life-years gained and the human capital and full income net present value of investment. We estimated the effects of stage at diagnosis, radiotherapy delivery system, and simultaneous HPV vaccination (75% coverage) up to a time horizon set at 2072.
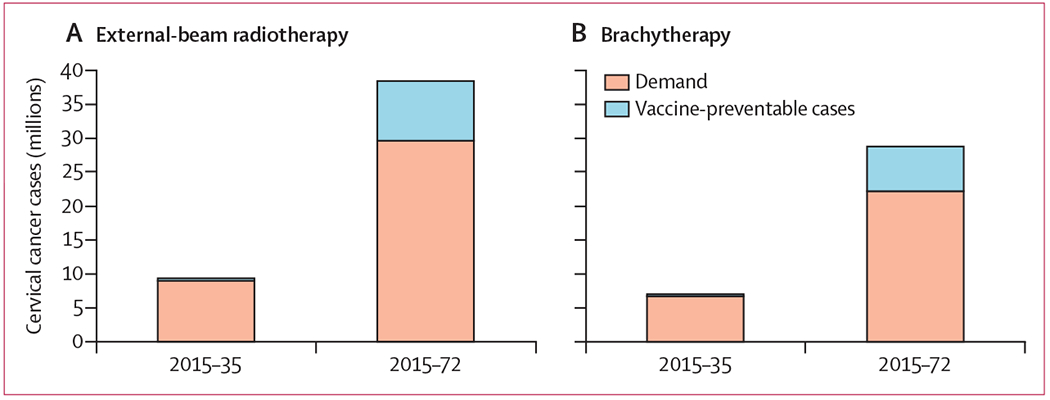
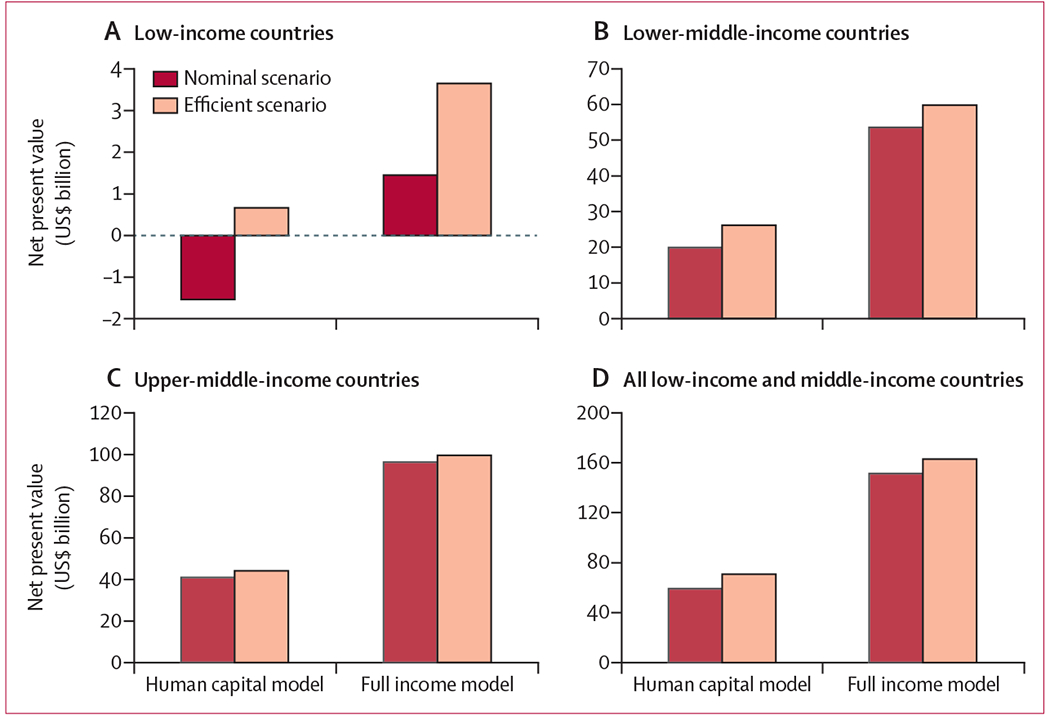
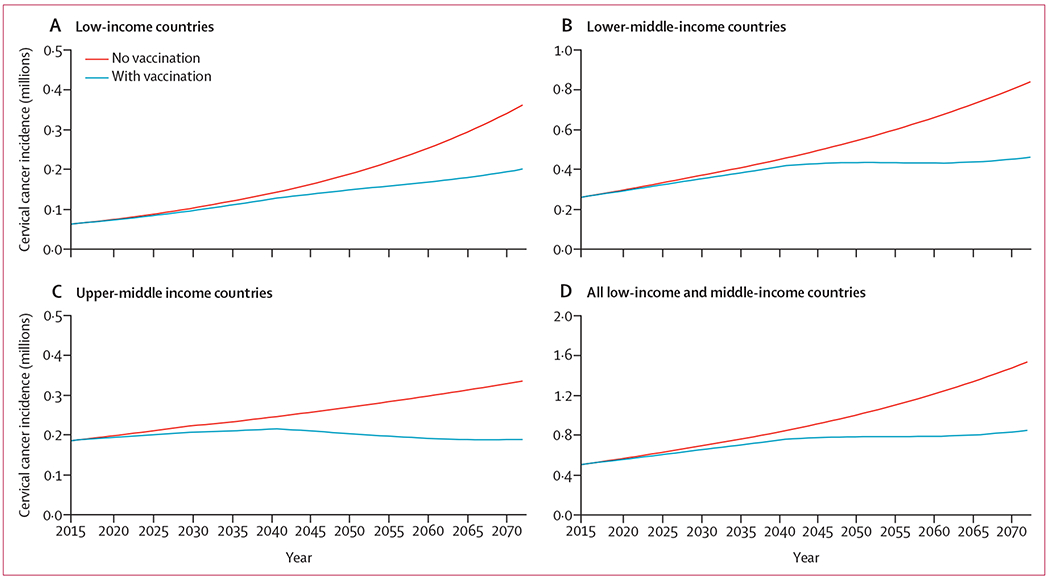
For the period from 2015 to 2035, we estimated that 9·4 million women in low-income and middle-income countries required treatment with external-beam radiotherapy, of which 7·0 million also required treatment with brachytherapy. Incremental scale-up of radiotherapy in these countries from 2015 to meet optimal radiotherapy demand by 2035 yielded 11·4 million life-years gained, $59·3 billion in human capital net present value (-$1·5 billion in low-income, $19·9 billion in lower-middle-income, and $40·9 billion in upper-middle-income countries), and $151·5 billion in full income net present value ($1·5 billion in low-income countries, $53·6 billion in lower-middle-income countries, and $96·4 billion in upper-middle-income countries). Benefits increased with advanced stage of cervical cancer and more efficient scale up of radiotherapy. Bivalent HPV vaccination of 12-year-old girls resulted in a 3·9% reduction in incident cases from 2015-2035. By 2072, when the first vaccinated cohort of girls reaches 70 years of age, vaccination yielded a 22·9% reduction in cervical cancer incidence, with 38·4 million requiring external-beam radiotherapy and 28·8 million requiring brachytherapy.
Effective cervical cancer control requires a comprehensive strategy. Even with HPV vaccination, radiotherapy treatment scale-up remains essential and produces large health benefits and a strong return on investment to countries at different levels of development.
None.
放射疗法是宫颈癌的标准治疗方法,但全球在获取放射疗法方面存在着重大差距,尤其是在低收入和中等收入国家。我们构建了一个 20 年放射疗法扩展模型,以评估在人乳头瘤病毒(HPV)疫苗接种背景下对治疗的长期需求。
我们应用全球癌症放射治疗工作队的投资框架,构建了一个模型,以评估中上收入、中下收入和低收入国家在 2015 年至 2035 年期间扩大宫颈癌外照射放射疗法和近距离放射疗法的健康和经济效益。我们估计了外照射放射疗法和近距离放射疗法的独特成本,并包括了对女性护理贡献的特定估值。模型结果为获得的生命年数以及投资的人力资本和总收入净现值。我们估计了诊断时的阶段、放射治疗输送系统以及同时进行的 HPV 疫苗接种(覆盖率 75%)的效果,直至设定在 2072 年的时间范围内。
在 2015 年至 2035 年期间,我们估计中低收入国家有 940 万妇女需要接受外照射放射疗法治疗,其中 700 万妇女还需要接受近距离放射疗法治疗。从 2015 年开始逐步扩大放射疗法的规模,以满足 2035 年最佳放射疗法的需求,这使得获得的生命年数增加了 1140 万,人力资本净现值为 593 亿美元(低收入国家为-15 亿美元,中下收入国家为 199 亿美元,中上收入国家为 409 亿美元),总收入净现值为 1515 亿美元(低收入国家为 15 亿美元,中下收入国家为 536 亿美元,中上收入国家为 964 亿美元)。随着宫颈癌的晚期发展和更有效的放射疗法扩展,效益增加。对 12 岁女孩进行二价 HPV 疫苗接种,将使 2015 年至 2035 年期间的发病病例减少 3.9%。到 2072 年,当第一批接种疫苗的女孩达到 70 岁时,疫苗接种将使宫颈癌的发病率降低 22.9%,需要接受外照射放射疗法的人数为 3840 万,需要接受近距离放射疗法的人数为 2880 万。
有效的宫颈癌控制需要综合战略。即使有 HPV 疫苗接种,放射疗法的治疗扩展仍然是必要的,并且会给不同发展水平的国家带来巨大的健康益处和强劲的投资回报。
无。