Department of Obstetrics and Gynecology, University of Amsterdam, Amsterdam UMC, Location AMC, Amsterdam, The Netherlands.
Center for Gynecologic Oncology Amsterdam, Department of Gynecologic Oncology, The Netherlands Cancer Institute/Antoni Van Leeuwenhoek Hospital, Amsterdam, The Netherlands.
Clin Exp Metastasis. 2020 Apr;37(2):293-304. doi: 10.1007/s10585-020-10024-4. Epub 2020 Feb 1.
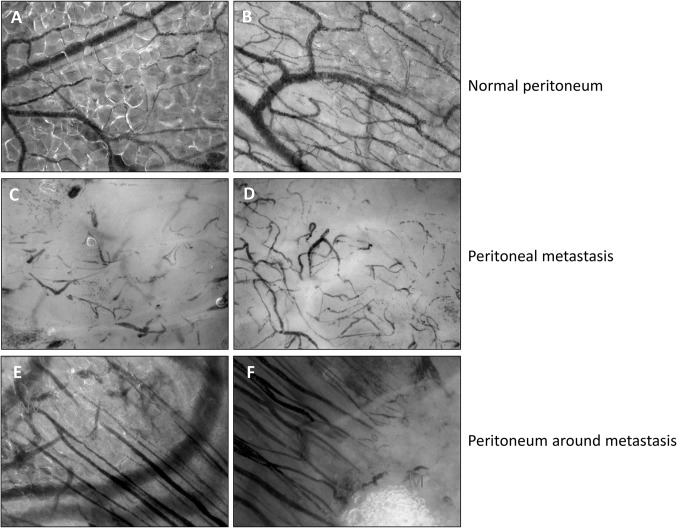
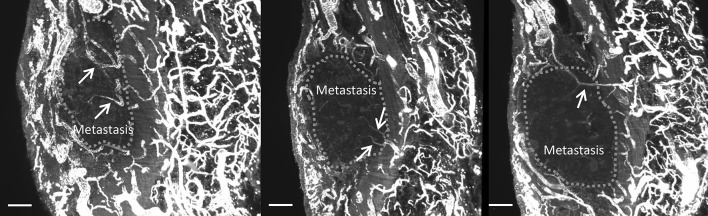
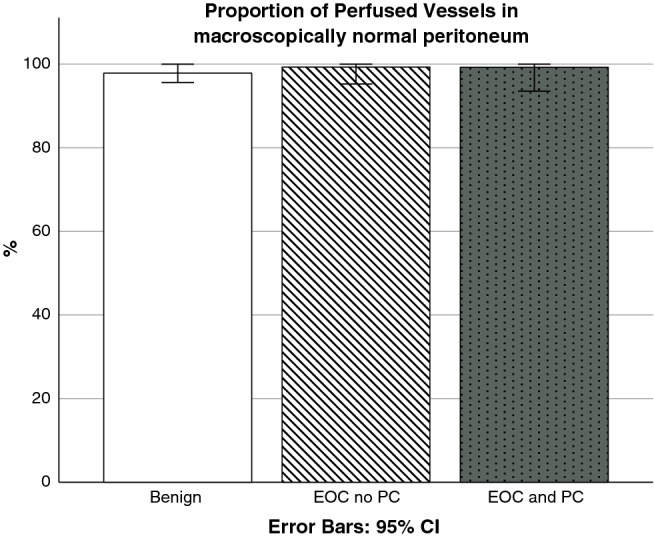
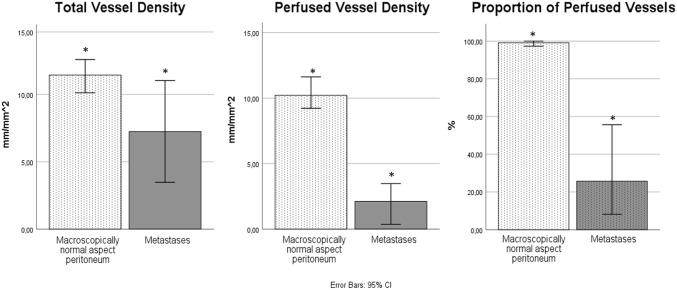
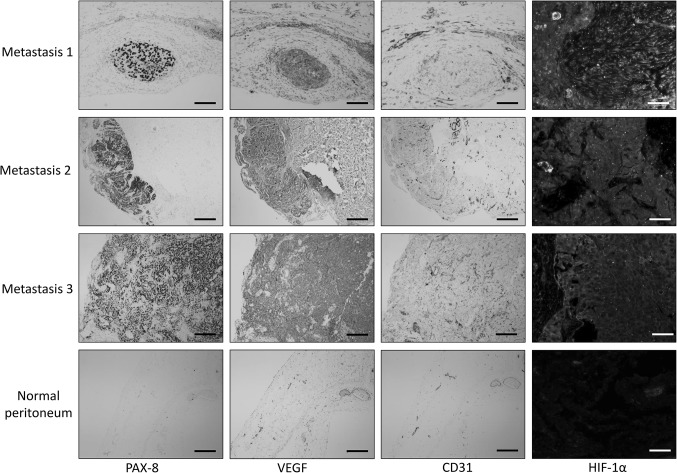
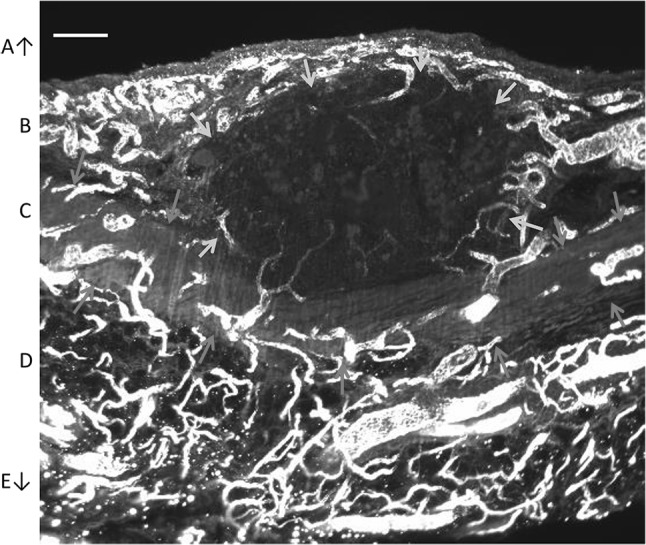
Most women with epithelial ovarian cancer (EOC) suffer from peritoneal carcinomatosis upon first clinical presentation. Extensive peritoneal carcinomatosis has a poor prognosis and its pathophysiology is not well understood. Although treatment with systemic intravenous chemotherapy is often initially successful, peritoneal recurrences occur regularly. We hypothesized that insufficient or poorly-perfused microvasculature may impair the therapeutic efficacy of systemic intravenous chemotherapy but may also limit expansive and invasive growth characteristic of peritoneal EOC metastases. In 23 patients with advanced EOC or suspicion thereof, we determined the angioarchitecture and perfusion of the microvasculature in peritoneum and in peritoneal metastases using incident dark field (IDF) imaging. Additionally, we performed immunohistochemical analysis and 3-dimensional (3D) whole tumor imaging using light sheet fluorescence microscopy of IDF-imaged tissue sites. In all metastases, microvasculature was present but the angioarchitecture was chaotic and the vessel density and perfusion of vessels was significantly lower than in unaffected peritoneum. Immunohistochemical analysis showed expression of vascular endothelial growth factor and hypoxia inducible factor 1α, and 3D imaging demonstrated vascular continuity between metastases and the vascular network of the peritoneum beneath the elastic lamina of the peritoneum. We conclude that perfusion of the microvasculature within metastases is limited, which may cause hypoxia, affect the behavior of EOC metastases on the peritoneum and limit the response of EOC metastases to systemic treatment.
大多数上皮性卵巢癌 (EOC) 患者在首次临床就诊时即患有腹膜癌病。广泛的腹膜癌病预后不良,其病理生理学尚不清楚。尽管全身静脉化疗的初始治疗通常有效,但腹膜复发经常发生。我们假设,微血管的不足或灌注不良可能会降低全身静脉化疗的疗效,但也可能限制腹膜 EOC 转移的扩张和侵袭性生长。在 23 名患有晚期 EOC 或疑似 EOC 的患者中,我们使用暗场成像 (IDF) 确定了腹膜和腹膜转移灶中微血管的血管结构和灌注。此外,我们还对 IDF 成像组织部位进行了光片荧光显微镜的免疫组织化学分析和 3 维(3D)全肿瘤成像。在所有转移灶中都存在微血管,但血管结构混乱,血管密度和血管灌注明显低于未受影响的腹膜。免疫组织化学分析显示血管内皮生长因子和缺氧诱导因子 1α的表达,3D 成像显示转移灶与腹膜弹性层下腹膜血管网络之间的血管连续性。我们得出结论,转移灶内微血管的灌注受限,这可能导致缺氧,影响 EOC 转移在腹膜上的行为,并限制 EOC 转移对全身治疗的反应。