Division of Cardiology Pauley Heart Center Virginia Commonwealth University Richmond VA.
Johnson Center for Critical Care and Pulmonary Research Virginia Commonwealth University Richmond VA.
J Am Heart Assoc. 2020 Feb 4;9(3):e014213. doi: 10.1161/JAHA.119.014213. Epub 2020 Jan 30.
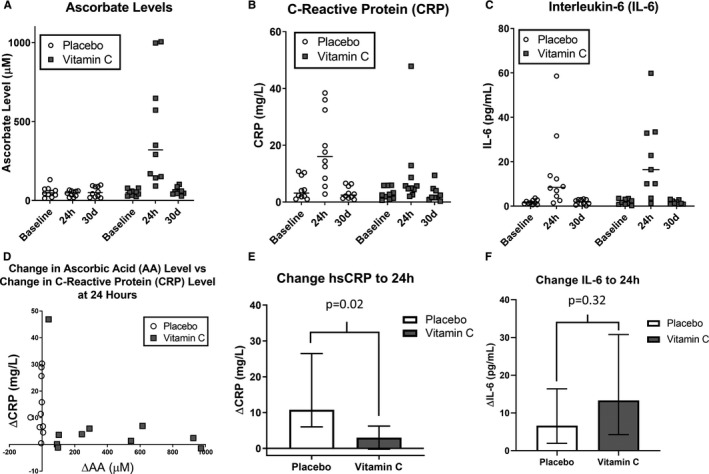
Background Catheter ablation is an effective treatment for atrial fibrillation (AF), but high levels of post-procedure inflammation predict adverse clinical events. Ascorbic acid (AA) has shown promise in reducing inflammation but is untested in this population. We sought to test the feasibility, safety, and preliminary effects on inflammatory biomarkers in the CITRIS-AF (Vitamin C Intravenous Treatment In the Setting of Atrial Fibrillation Ablation) pilot study. Methods and Results Patients scheduled to undergo AF ablation (N=20) were randomized 1:1 to double-blinded treatment with AA (200 mg/kg divided over 24 hours) or placebo. C-reactive protein and interleukin-6 levels were obtained before the first infusion and repeated at 24 hours and 30 days. Pain levels within 24 hours and early recurrence of AF within 90 days were recorded. Median and interquartile range were aged 63 (56-70) years, 13 (65%) men, and 18 (90%) white. Baseline data were similar between the 2 groups except ejection fraction. Baseline C-reactive protein levels were 2.56 (1.47-5.87) mg/L and similar between groups (=0.48). Change in C-reactive protein from baseline to 24 hours was +10.79 (+6.56-23.19) mg/L in the placebo group and +3.01 (+0.40-5.43) mg/L in the AA group (=0.02). Conversely, change in interleukin-6 was numerically higher in the AA group, though not statistically significant (=0.32). One patient in each arm developed pericarditis; no adverse events related to the infusions were seen. There were no significant differences between aggregated post-procedure pain levels within 24 hours or early recurrence of AF (both >0.05). Conclusions High-dose AA is safe and well tolerated at the time of AF ablation and may be associated with a blunted rise in C-reactive protein, although consistent findings were not seen in interleukin-6 levels. Further studies are needed to validate these findings and explore the potential benefit in improving clinically relevant outcomes. Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier: NCT03148236.
背景 导管消融术是治疗心房颤动(AF)的有效方法,但术后炎症水平高预示着不良临床事件。抗坏血酸(AA)在减轻炎症方面显示出前景,但在该人群中尚未得到验证。我们旨在测试 CITRIS-AF(维生素 C 静脉治疗在心房颤动消融中的应用)试验研究中的可行性、安全性和对炎症生物标志物的初步影响。
方法和结果 计划接受 AF 消融的患者(N=20)按 1:1 随机分为 AA(200mg/kg 分 24 小时输注)或安慰剂组,进行双盲治疗。在第一次输注前和 24 小时及 30 天时获取 C 反应蛋白和白细胞介素-6 水平。记录 24 小时内的疼痛程度和 90 天内 AF 的早期复发情况。
中位数和四分位距为 63(56-70)岁,13(65%)名男性,18(90%)名白人。两组间的基线数据相似,除射血分数外。两组间的基线 C 反应蛋白水平分别为 2.56(1.47-5.87)mg/L 和 2.56(1.47-5.87)mg/L(=0.48)。安慰剂组 24 小时时 C 反应蛋白从基线的变化为+10.79(+6.56-23.19)mg/L,AA 组为+3.01(+0.40-5.43)mg/L(=0.02)。相反,AA 组白细胞介素-6 的变化虽然没有统计学意义,但数值更高(=0.32)。两组各有 1 例患者发生心包炎;未观察到与输注相关的不良事件。两组 24 小时内聚合后的术后疼痛水平或 AF 的早期复发无显著差异(均>0.05)。
结论 在进行 AF 消融术时,高剂量 AA 是安全且耐受良好的,可能与 C 反应蛋白的升高幅度降低有关,尽管白细胞介素-6 水平未见一致的发现。需要进一步的研究来验证这些发现,并探讨改善临床相关结局的潜在益处。