Department of Cardiothoracic Surgery, Jena, Germany.
Center for Sepsis Control and Care, Jena, Germany.
PLoS One. 2020 Feb 3;15(2):e0228286. doi: 10.1371/journal.pone.0228286. eCollection 2020.
More than 50% of patients with infective endocarditis (IE) develop an indication for surgery. Despite its benefit, surgery is associated with a high incidence of multiple organ dysfunction syndrome (MODS) and mortality, which may be linked to increased release of inflammatory mediators during cardiopulmonary bypass (CPB). We therefore assessed plasma cytokine profiles in patients undergoing valve surgery with or without IE.
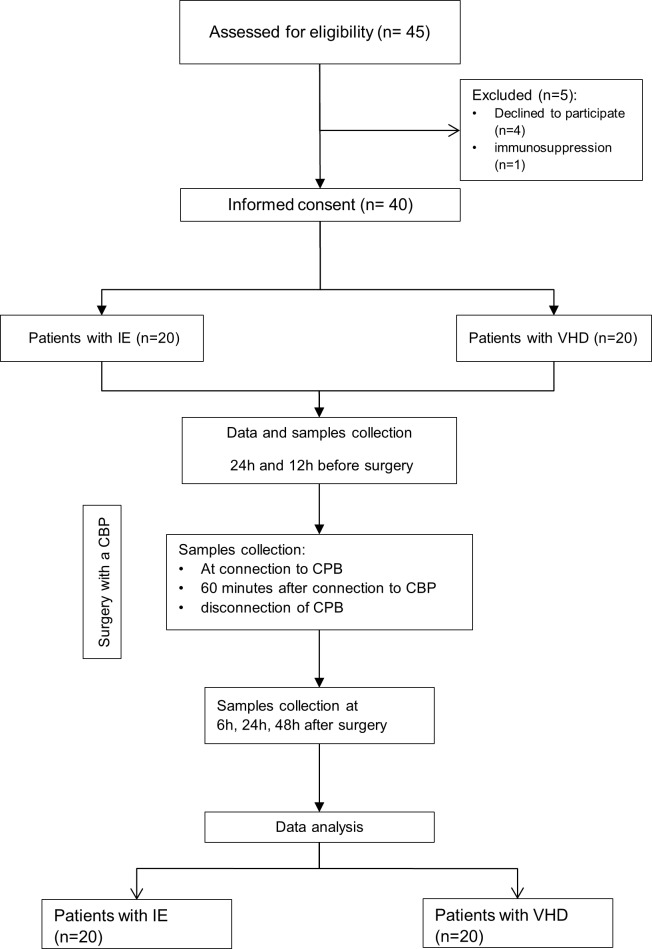
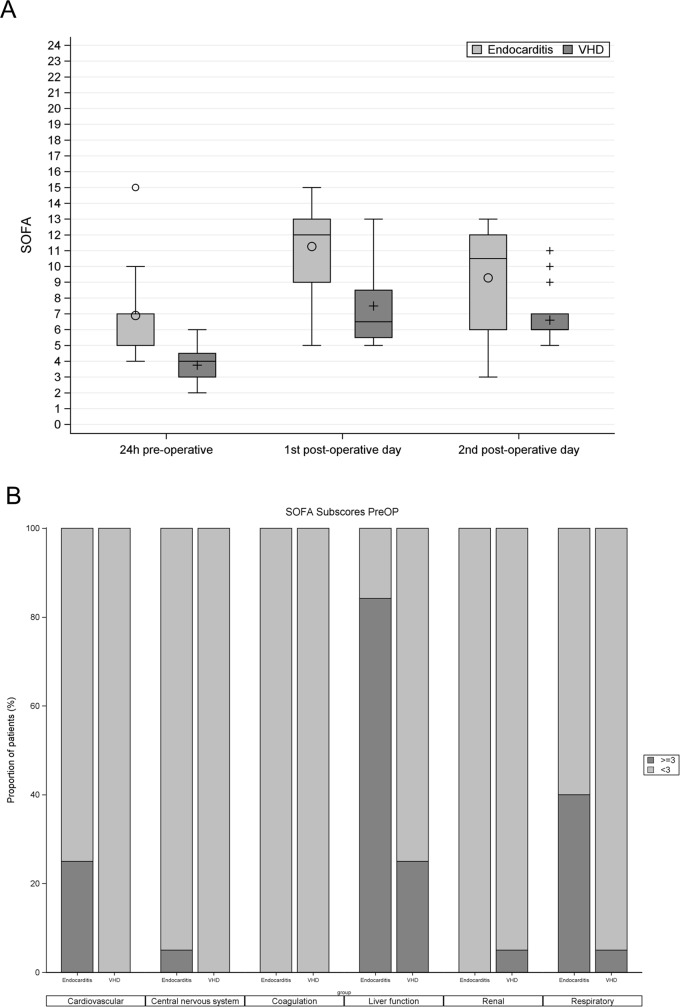
We performed a prospective case-control pilot study comparing patients undergoing cardiac valve surgery with or without IE. Plasma profiles of inflammatory mediators were measured at 7 defined time points and reported as median (interquartile). The degree of MODS was measured using sequential organ failure assessment (SOFA) score.
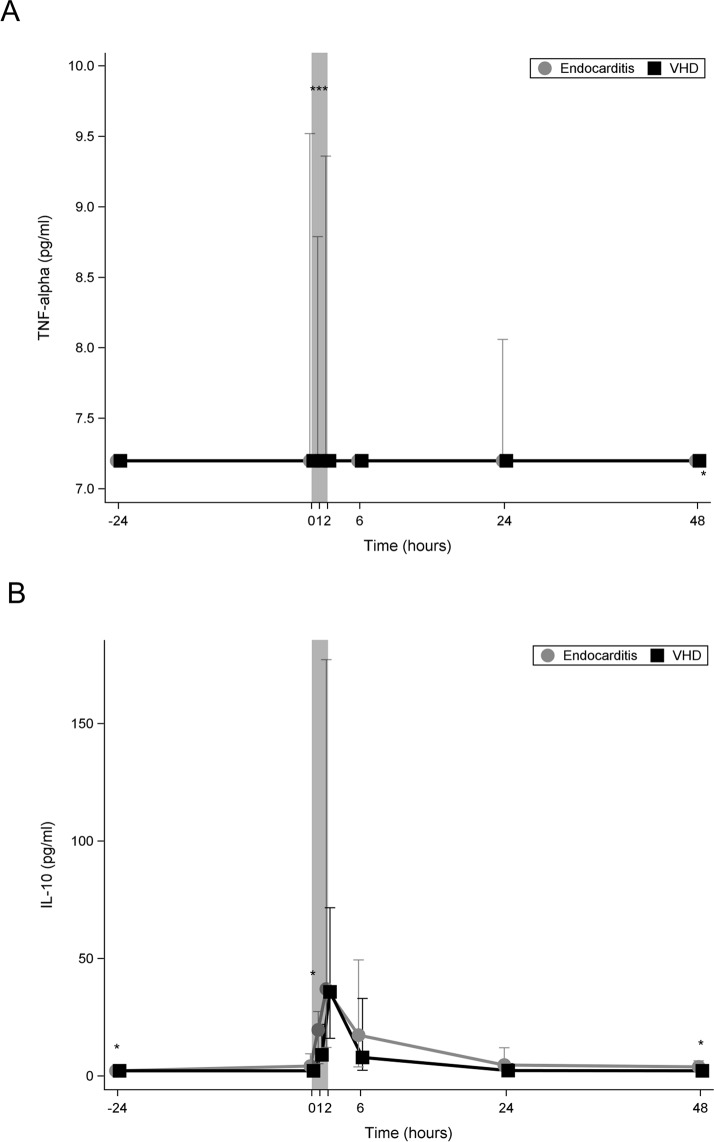
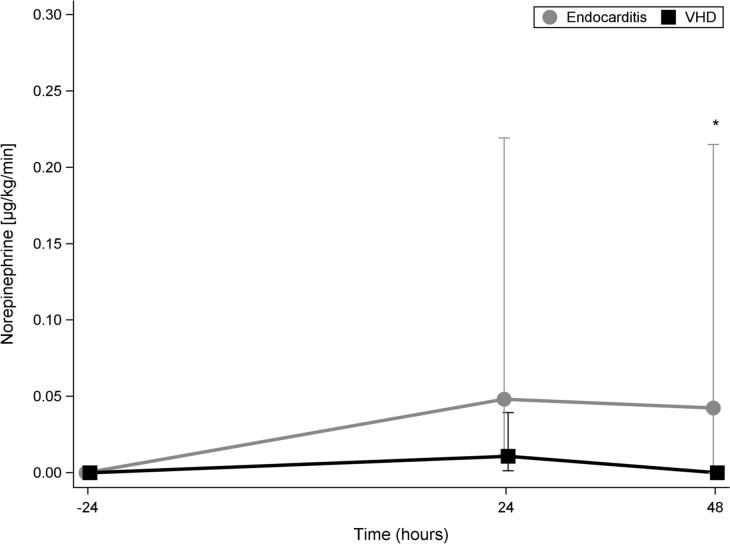
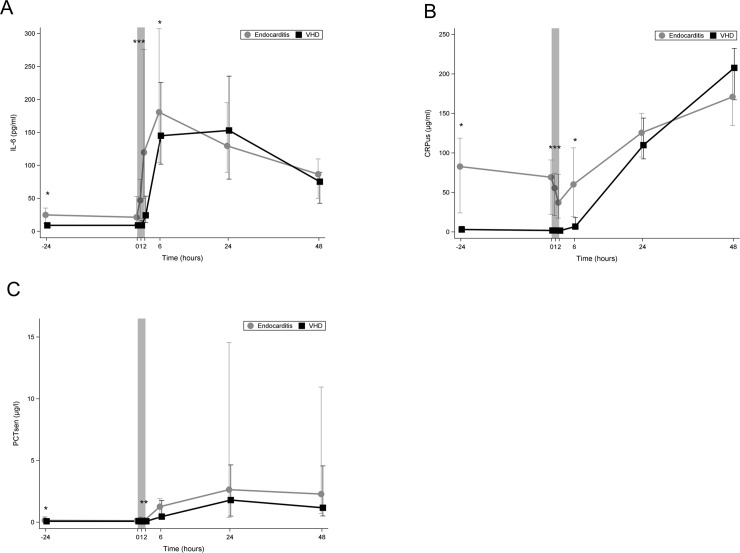
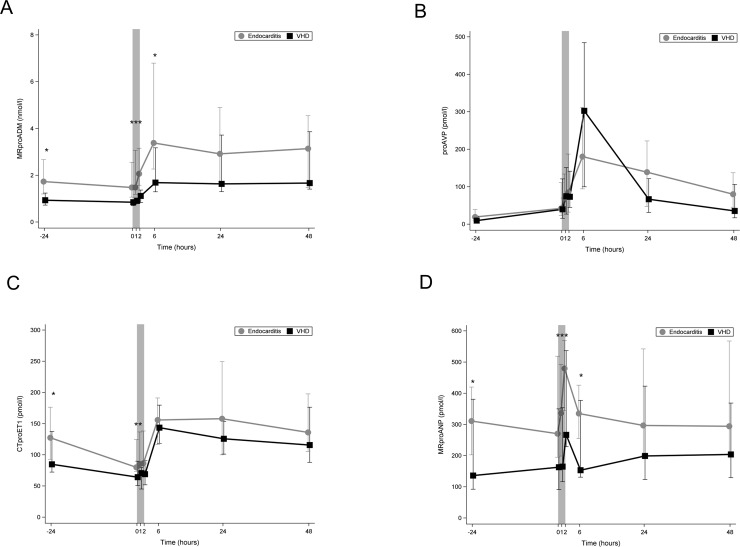
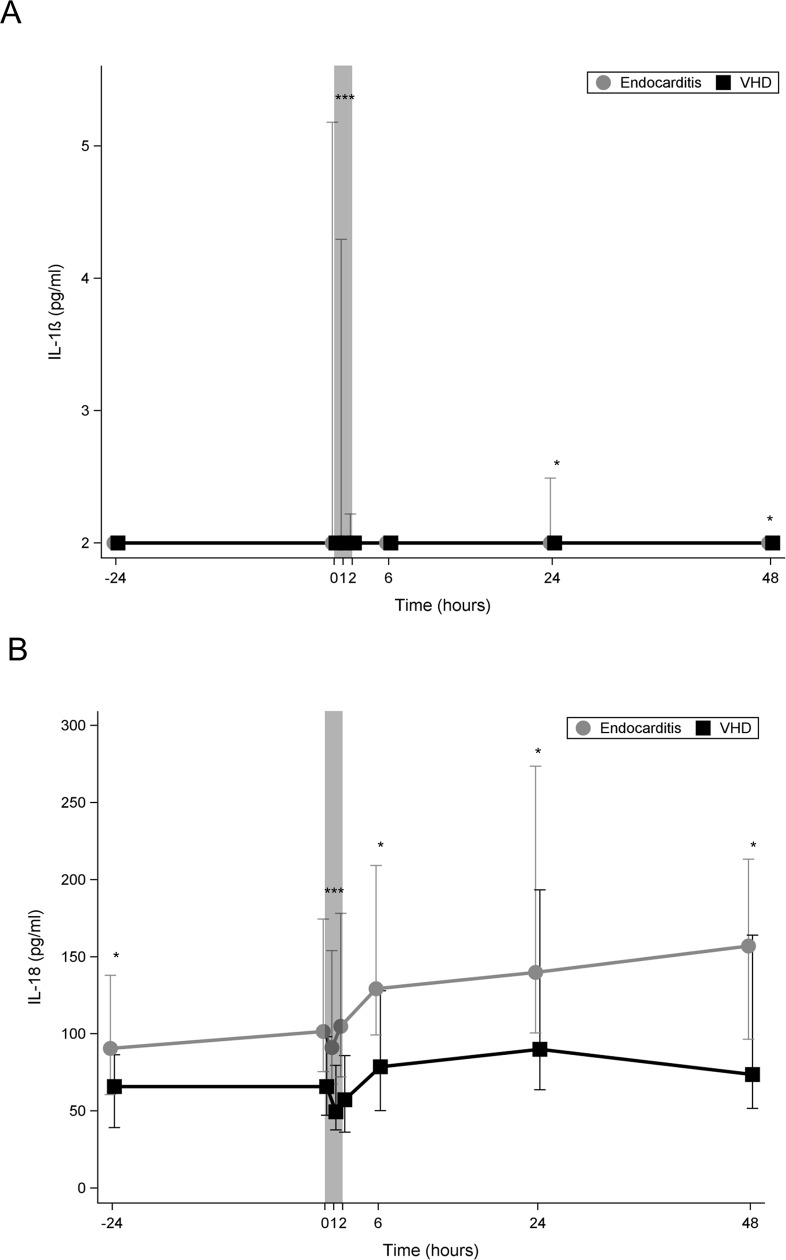
Between May and December 2016 we included 40 patients (20 in each group). Both groups showed similar distribution of age and gender. Patients with IE had higher preoperative SOFA (6.9± 2.6 vs 3.8 ± 1.1, p<0.001) and operative risk scores (EuroSCORE II 18.6±17.4 vs. 1.8±1.3, p<0.001). In-hospital mortality was higher in IE patients (35% vs. 5%; p<0.001). Multiple organ failure was the cause of death in all non-survivors. At the end of CPB, median levels of following inflammatory mediators were higher in IE compared to control group: IL-6 (119.73 (226.49) vs. 24.48 (40.09) pg/ml, p = 0.001); IL-18 (104.82 (105.99) vs. 57.30 (49.53) pg/ml, p<0.001); Mid-regional pro-adrenomedullin (MR-proADM) (2.06 (1.58) vs. 1.11 (0.53) nmol/L, p = 0.003); MR- pro-atrial natriuretic peptide (MR-proANP) (479.49 (224.74) vs. 266.55 (308.26) pmol/l, p = 0.028). IL-1β and TNF- α were only detectable in IE patients and first after starting CPB. Plasma levels of IL-6, IL-18, MRproADM, and MRproANP during CPB were significantly lower in survivors than in those who died.
The presence of infective endocarditis during cardiac valve surgery is associated with increased inflammatory response as evident by higher plasma cytokine levels and other inflammatory mediators. Actively reducing inflammatory response appears to be a plausible therapeutic concept.
ClinicalTrials.gov, ID: NCT02727413.
超过 50%的感染性心内膜炎(IE)患者需要手术治疗。尽管手术有益,但它与多器官功能障碍综合征(MODS)和死亡率的高发生率相关,这可能与体外循环(CPB)期间炎症介质的释放增加有关。因此,我们评估了接受心脏瓣膜手术的 IE 患者和非 IE 患者的血浆细胞因子谱。
我们进行了一项前瞻性病例对照试点研究,比较了接受心脏瓣膜手术的 IE 患者和非 IE 患者。在 7 个规定的时间点测量炎症介质的血浆谱,并以中位数(四分位距)报告。使用序贯器官衰竭评估(SOFA)评分测量 MODS 的程度。
2016 年 5 月至 12 月期间,我们纳入了 40 名患者(每组 20 名)。两组的年龄和性别分布相似。IE 患者的术前 SOFA(6.9±2.6 与 3.8 ±1.1,p<0.001)和手术风险评分(EuroSCORE II 18.6±17.4 与 1.8±1.3,p<0.001)更高。IE 患者的住院死亡率更高(35%与 5%;p<0.001)。所有非幸存者的死亡原因都是多器官衰竭。在 CPB 结束时,IE 组与对照组相比,以下炎症介质的中位水平更高:白细胞介素 6(119.73(226.49)与 24.48(40.09)pg/ml,p=0.001);白细胞介素 18(104.82(105.99)与 57.30(49.53)pg/ml,p<0.001);中肽前肾上腺髓质素(MR-proADM)(2.06(1.58)与 1.11(0.53)nmol/L,p=0.003);MR- 心房利钠肽前肽(MR-proANP)(479.49(224.74)与 266.55(308.26)pmol/l,p=0.028)。白细胞介素 1β和肿瘤坏死因子-α仅在 IE 患者中可检测到,且仅在开始 CPB 后才可检测到。CPB 期间,存活者的白细胞介素 6、白细胞介素 18、MR-proADM 和 MR-proANP 血浆水平明显低于死亡者。
心脏瓣膜手术期间存在感染性心内膜炎与更高的细胞因子水平和其他炎症介质表明炎症反应增强有关。积极降低炎症反应似乎是一种合理的治疗概念。
ClinicalTrials.gov,ID:NCT02727413。