Centre for Big Data Research in Health, Faculty of Medicine, University of New South Wales (UNSW), Sydney, NSW, 2052, Australia.
School of Population and Global Health, University of Western Australia, Perth, Australia.
BMC Med. 2020 Feb 5;18(1):15. doi: 10.1186/s12916-019-1472-9.
Varenicline, bupropion and nicotine replacement therapy (NRT) are three effective pharmacotherapies for smoking cessation, but data about their safety in pregnancy are limited. We assessed the risk of adverse perinatal outcomes and major congenital anomalies associated with the use of these therapies in pregnancy in Australia.
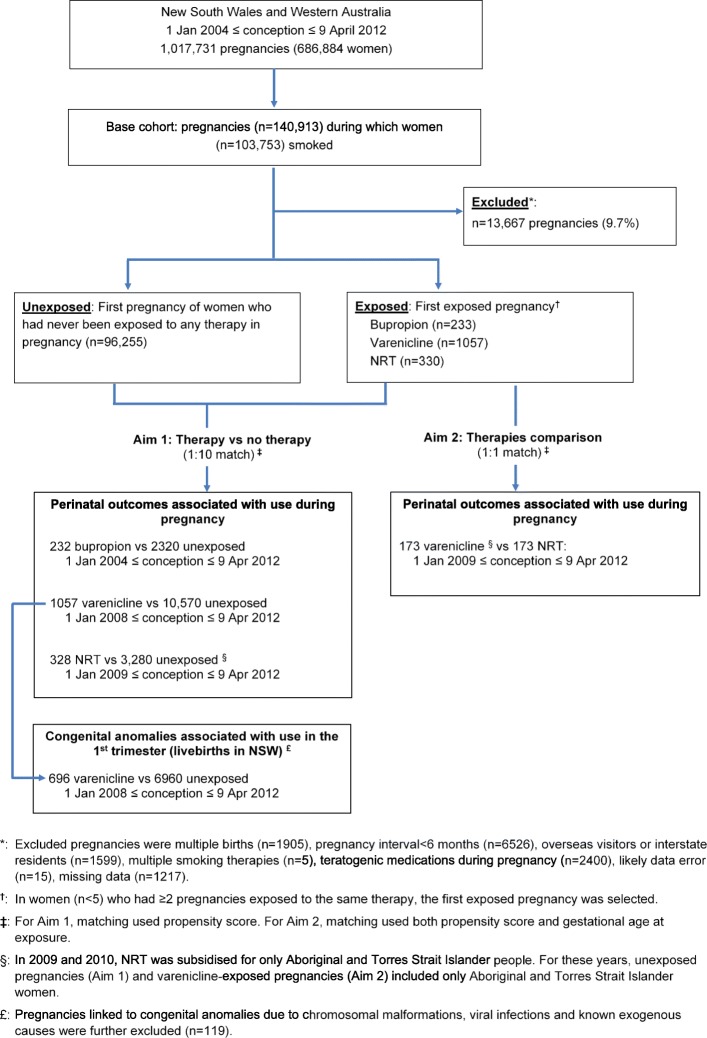
Perinatal data for 1,017,731 deliveries (2004 to 2012) in New South Wales and Western Australia were linked to pharmaceutical dispensing, hospital admission and death records. We identified 97,875 women who smoked during pregnancy; of those, 233, 330 and 1057 were exposed to bupropion, NRT and varenicline in pregnancy, respectively. Propensity scores were used to match exposed women to those who were unexposed to any smoking therapy (1:10 ratio). Propensity scores and gestational age at exposure were used to match varenicline-exposed to NRT-exposed women (1:1 ratio). Time-dependent Cox proportional hazards models estimated hazard ratios (HR) with 95% confidence intervals (95% CI) for any adverse perinatal event (a composite of 10 unfavourable maternal and neonatal outcomes) and any major congenital anomaly.
The risk of any adverse perinatal event was not significantly different between bupropion-exposed and unexposed women (39.2% versus 39.3%, HR 0.93, 95% CI 0.73-1.19) and between NRT-exposed and unexposed women (44.8% vs 46.3%, HR 1.02, 95% CI 0.84-1.23), but it was significantly lower in women exposed to varenicline (36.9% vs 40.1%, HR 0.86, 95% CI 0.77-0.97). Varenicline-exposed infants were less likely than unexposed infants to be born premature (6.5% vs 8.9%, HR 0.72, 95% CI 0.56-0.92), be small for gestational age (11.4% vs 15.4%, HR 0.68, 95% CI 0.56-0.83) and have severe neonatal complications (6.6% vs 8.2%, HR 0.74, 95% CI 0.57-0.96). Among infants exposed to varenicline in the first trimester, 2.9% had a major congenital anomaly (3.5% in unexposed infants, HR 0.91, 95% CI 0.72-1.15). Varenicline-exposed women were less likely than NRT-exposed women to have an adverse perinatal event (38.7% vs 51.4%, HR 0.58, 95% CI 0.33-1.05).
Pregnancy exposure to smoking cessation pharmacotherapies does not appear to be associated with an increased risk of adverse birth outcomes. Lower risk of adverse birth outcomes in varenicline-exposed pregnancies is inconsistent with recommendations that NRT be used in preference to varenicline.
伐尼克兰、安非他酮和尼古丁替代疗法(NRT)是三种有效的戒烟药物疗法,但关于这些药物在怀孕期间安全性的数据有限。我们评估了在澳大利亚这些疗法在怀孕期间使用与不良围产期结局和主要先天畸形相关的风险。
新南威尔士州和西澳大利亚州的 1017731 例分娩(2004 年至 2012 年)的围产期数据与药品配药、住院和死亡记录相关联。我们确定了 97875 名怀孕期间吸烟的女性;其中,233、330 和 1057 名女性分别在怀孕期间暴露于安非他酮、NRT 和伐尼克兰。使用倾向评分将暴露于药物的女性与未暴露于任何戒烟疗法的女性(1:10 比例)相匹配。使用倾向评分和暴露时的孕龄将暴露于伐尼克兰的女性与暴露于 NRT 的女性相匹配(1:1 比例)。时间依赖性 Cox 比例风险模型估计了任何不良围产期事件(10 种不良母婴结局的综合)和任何主要先天畸形的风险比(HR)及其 95%置信区间(95%CI)。
暴露于安非他酮的女性与未暴露于药物的女性(39.2%与 39.3%,HR 0.93,95%CI 0.73-1.19)和暴露于 NRT 的女性与未暴露于药物的女性(44.8%与 46.3%,HR 1.02,95%CI 0.84-1.23)的不良围产期事件风险无显著差异,但暴露于伐尼克兰的女性的风险显著降低(36.9%与 40.1%,HR 0.86,95%CI 0.77-0.97)。暴露于伐尼克兰的婴儿比未暴露于药物的婴儿更不可能早产(6.5%与 8.9%,HR 0.72,95%CI 0.56-0.92)、胎龄较小(11.4%与 15.4%,HR 0.68,95%CI 0.56-0.83)和出现严重新生儿并发症(6.6%与 8.2%,HR 0.74,95%CI 0.57-0.96)。在暴露于伐尼克兰的第一个三个月的婴儿中,有 2.9%患有主要先天畸形(未暴露于药物的婴儿为 3.5%,HR 0.91,95%CI 0.72-1.15)。暴露于伐尼克兰的女性与暴露于 NRT 的女性相比,不良围产期事件的风险较低(38.7%与 51.4%,HR 0.58,95%CI 0.33-1.05)。
怀孕期间接触戒烟药物疗法似乎不会增加不良出生结局的风险。暴露于伐尼克兰的妊娠中不良出生结局的风险降低与推荐使用 NRT 而不是伐尼克兰不一致。