Tsivgoulis Georgios, Saqqur Maher, Sharma Vijay K, Brunser Alejandro, Eggers Jürgen, Mikulik Robert, Katsanos Aristeidis H, Sergentanis Theodore N, Vadikolias Konstantinos, Perren Fabienne, Rubiera Marta, Bavarsad Shahripour Reza, Nguyen Huy Thang, Martínez-Sánchez Patricia, Safouris Apostolos, Heliopoulos Ioannis, Shuaib Ashfaq, Derksen Carol, Voumvourakis Konstantinos, Psaltopoulou Theodora, Alexandrov Anne W, Alexandrov Andrei V
Department of Neurology, University of Tennessee Health Science Center, Memphis, TN, USA.
Second Department of Neurology, Attikon University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece.
J Stroke. 2020 Jan;22(1):130-140. doi: 10.5853/jos.2019.01648. Epub 2020 Jan 31.
Although onset-to-treatment time is associated with early clinical recovery in acute ischemic stroke (AIS) patients treated with intravenous tissue plasminogen activator (tPA), the effect of the timing of tPA-induced recanalization on functional outcomes remains debatable.
We conducted a multicenter, prospective observational cohort study to determine whether early (within 1-hour from tPA-bolus) complete or partial recanalization assessed during 2-hour real-time transcranial Doppler monitoring is associated with improved outcomes in patients with proximal occlusions. Outcome events included dramatic clinical recovery (DCR) within 2 and 24-hours from tPA-bolus, 3-month mortality, favorable functional outcome (FFO) and functional independence (FI) defined as modified Rankin Scale (mRS) scores of 0-1 and 0-2 respectively.
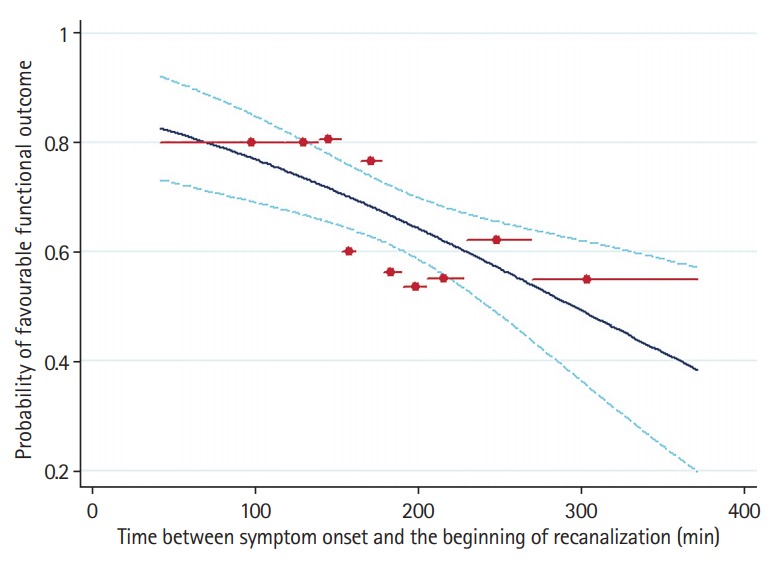
We enrolled 480 AIS patients (mean age 66±15 years, 60% men, baseline National Institutes of Health Stroke Scale score 15). Patients with early recanalization (53%) had significantly (P<0.001) higher rates of DCR at 2-hour (54% vs. 10%) and 24-hour (63% vs. 22%), 3-month FFO (67% vs. 28%) and FI (81% vs. 39%). Three-month mortality rates (6% vs. 17%) and distribution of 3-month mRS scores were significantly lower in the early recanalization group. After adjusting for potential confounders, early recanalization was independently associated with higher odds of 3-month FFO (odds ratio [OR], 6.19; 95% confidence interval [CI], 3.88 to 9.88) and lower likelihood of 3-month mortality (OR, 0.34; 95% CI, 0.17 to 0.67). Onset to treatment time correlated to the elapsed time between tPA-bolus and recanalization (unstandardized linear regression coefficient, 0.13; 95% CI, 0.06 to 0.19).
Earlier tPA treatment after stroke onset is associated with faster tPA-induced recanalization. Earlier onset-to-recanalization time.
in improved functional recovery and survival in AIS patients with proximal intracranial occlusions.
尽管在接受静脉注射组织型纤溶酶原激活剂(tPA)治疗的急性缺血性卒中(AIS)患者中,从发病到治疗的时间与早期临床恢复相关,但tPA诱导再通的时机对功能结局的影响仍存在争议。
我们进行了一项多中心、前瞻性观察队列研究,以确定在2小时实时经颅多普勒监测期间评估的早期(tPA推注后1小时内)完全或部分再通是否与近端闭塞患者的预后改善相关。结局事件包括tPA推注后2小时和24小时内的显著临床恢复(DCR)、3个月死亡率、良好功能结局(FFO)和功能独立性(FI),分别定义为改良Rankin量表(mRS)评分为0 - 1和0 - 2。
我们纳入了480例AIS患者(平均年龄66±15岁,60%为男性,基线美国国立卫生研究院卒中量表评分为15)。早期再通的患者(53%)在2小时(54%对10%)和24小时(63%对22%)时的DCR率、3个月FFO(67%对28%)和FI(81%对39%)显著更高(P<0.001)。早期再通组的3个月死亡率(6%对17%)和3个月mRS评分分布显著更低。在调整潜在混杂因素后,早期再通与3个月FFO的较高几率(优势比[OR],6.9;95%置信区间[CI],3.88至9.88)和3个月死亡率的较低可能性(OR,0.34;95%CI,0.17至0.67)独立相关。从发病到治疗的时间与tPA推注到再通的时间间隔相关(非标准化线性回归系数,0.13;95%CI,0.06至0.19)。
卒中发作后更早的tPA治疗与tPA诱导的更快再通相关。更早的从发病到再通时间。
在有近端颅内闭塞的AIS患者中改善了功能恢复和生存率。