Department of Internal Medicine, National Health Insurance Service Medical Center, Ilsan Hospital, Goyangshi, Gyeonggi-do, Republic of Korea.
Research and Analysis Team, National Health Insurance Service Medical Center, Ilsan Hospital, Goyangshi, Gyeonggi-do, Republic of Korea.
Mayo Clin Proc. 2020 Feb;95(2):231-242. doi: 10.1016/j.mayocp.2019.09.028.
To examine the association between income level and incident chronic kidney disease (CKD) in adults with normal baseline kidney function.
We studied the association between income level categorized into deciles and incident CKD in a national cohort comprised of 7,405,715 adults who underwent National Health Insurance Service health examinations during January 1, 2009, to December 31, 2015, with baseline estimated glomerular filtration rates (eGFRs) ≥60 mL/min/1.73 m. Incident CKD was defined as de novo development of eGFR <60 mL/min/1.73 m (model 1) or ≥25% decline in eGFR from baseline values accompanied by eGFR <60 mL/min/1.73 m (model 2).
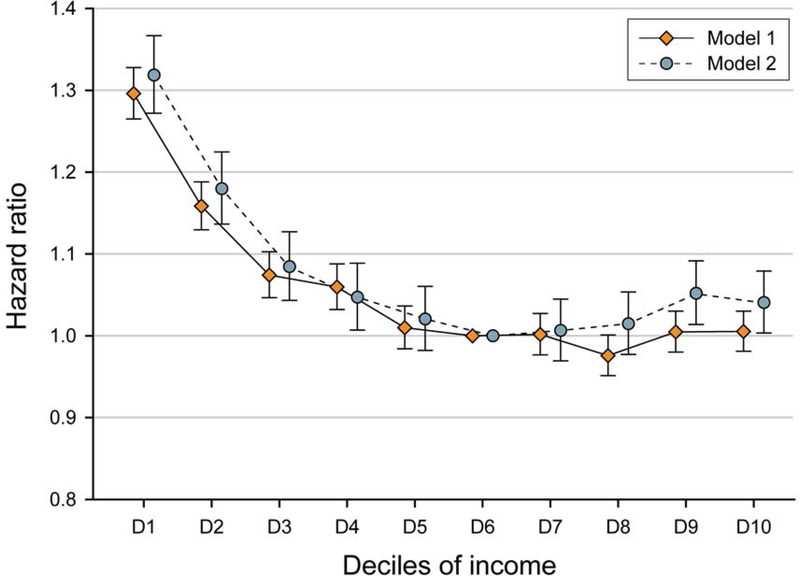
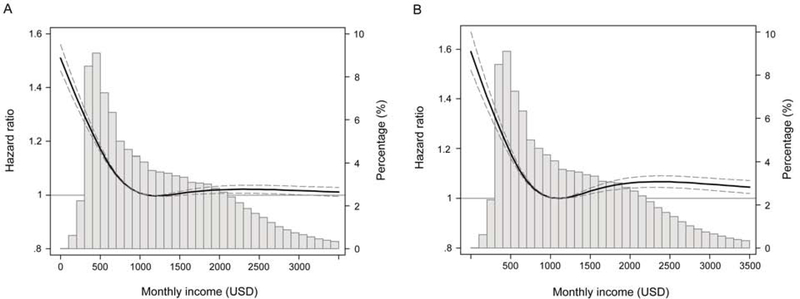
During a median follow-up of 4.8 years, there were 122,032 of 7,405,715 (1.65%) and 55,779 of 7,405,715 (0.75%) incident CKD events based on model 1 and 2 definitions, respectively. Compared with income levels in the sixth decile, there was an inverse association between lower income level and higher risk for CKD up to the fourth decile, above which no additional reduction (model 1) or slightly higher risk for CKD (model 2) was observed at higher income levels. The multivariable-adjusted hazard ratios from the lowest to fourth deciles were 1.30 (95% CI, 1.26-1.33), 1.16 (95% CI, 1.13-1.19), 1.07 (95% CI, 1.05-1.10), and 1.06 (95% CI, 1.03-1.09) in model 1 and 1.32 (95% CI, 1.27-1.37), 1.18 (95% CI, 1.14-1.22), 1.08 (95% CI, 1.04-1.13), and 1.05 (95% CI, 1.01-1.09) in model 2, respectively. These associations persisted across various subgroups of age, sex, and comorbidity status.
In this large nationwide cohort, lower income levels were associated with higher risk for incident CKD.
探讨基线肾功能正常的成年人中,收入水平与慢性肾脏病(CKD)发病的相关性。
我们研究了一个全国性队列中收入水平(分为十等份)与 CKD 发病的相关性,该队列包括 7405715 名在 2009 年 1 月 1 日至 2015 年 12 月 31 日期间接受国民健康保险服务健康检查的成年人,基线估算肾小球滤过率(eGFR)≥60mL/min/1.73m。新发 CKD 定义为 eGFR<60mL/min/1.73m(模型 1)或 eGFR 较基线值下降≥25%并伴有 eGFR<60mL/min/1.73m(模型 2)。
在中位随访 4.8 年期间,根据模型 1 和 2 的定义,7405715 例患者中有 122032 例(1.65%)和 55779 例(0.75%)发生 CKD 事件。与第六分位数的收入水平相比,收入水平较低与 CKD 风险增加呈负相关,直到第四分位数,此后收入水平较高时,CKD 风险未见进一步降低(模型 1)或略升高(模型 2)。最低到第四分位数的多变量调整后危险比分别为 1.30(95%CI,1.26-1.33)、1.16(95%CI,1.13-1.19)、1.07(95%CI,1.05-1.10)和 1.06(95%CI,1.03-1.09)(模型 1)和 1.32(95%CI,1.27-1.37)、1.18(95%CI,1.14-1.22)、1.08(95%CI,1.04-1.13)和 1.05(95%CI,1.01-1.09)(模型 2)。这些关联在不同年龄、性别和合并症状态的亚组中均持续存在。
在这个大型全国性队列中,较低的收入水平与较高的 CKD 发病风险相关。