Sharma Yash Paul, Krishnappa Darshan, Kanabar Kewal, Kasinadhuni Ganesh, Sharma Rakesh, Kishore Kamal, Mehrotra Saurabh, Santosh Krishna, Gupta Ankur, Panda Prashant
Department of Cardiology, Advanced Cardiac Centre (ACC), Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, 160012, India.
Department of Cardiology, Advanced Cardiac Centre (ACC), Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, 160012, India.
Indian Heart J. 2019 Sep-Oct;71(5):387-393. doi: 10.1016/j.ihj.2019.11.256. Epub 2019 Nov 21.
Delayed presentation after ST-elevation myocardial infarction (STEMI) and complicated by cardiogenic shock (CS-STEMI) is commonly encountered in developing countries and is a challenging scenario because of a delay in revascularization resulting in infarction of a large amount of the myocardium. We aimed to assess the clinical characteristics, angiographic profile, and predictors of outcome in patients with a delayed presentation after CS-STEMI.
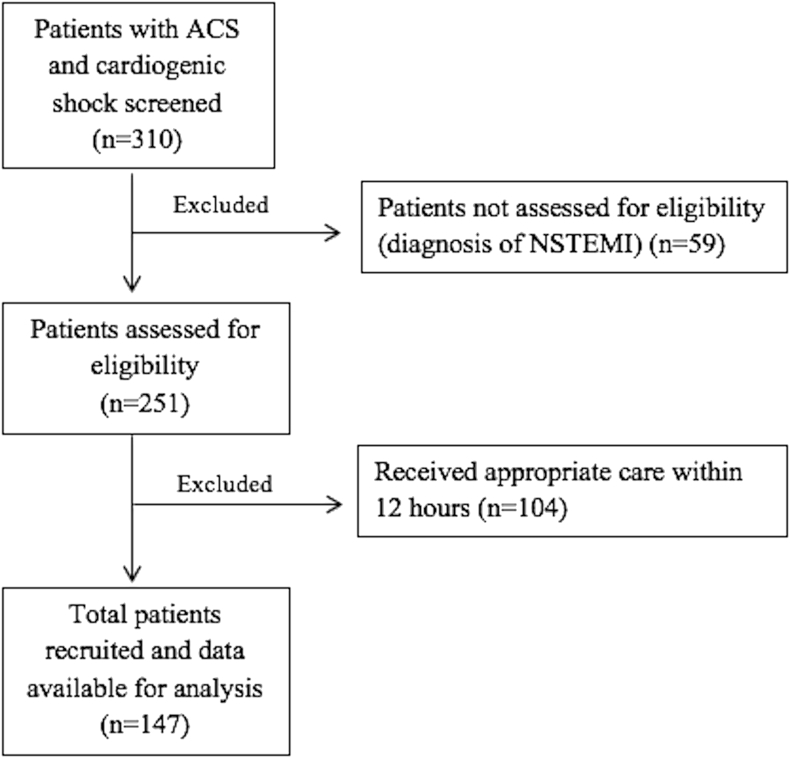
A total of 147 patients with CS-STEMI with time to appropriate medical care ≥12 h after symptom onset were prospectively recruited at a tertiary referral center.
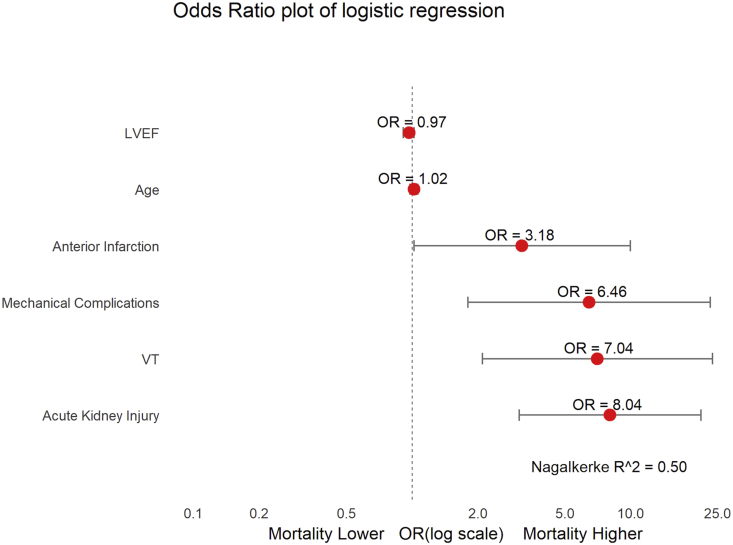
The median time to appropriate care was 24 h (interquartile range 18-48 h). The mean age was 58.7 ± 11.1 years. Left ventricular pump failure was the leading cause of shock (67.3%), whereas mechanical complications accounted for 14.9% and right ventricular infarction for 13.6% of cases. The overall in-hospital mortality was 42.9%. Acute kidney injury [Odds ratio (OR) 8.04; 95% confidence intervals (CI) 3.08-20.92], ventricular tachycardia (OR 7.04; CI 2.09-23.63), mechanical complications (OR 6.46; CI 1.80-23.13), and anterior infarction (OR 3.18; CI 1.01-9.97) were independently associated with an increased risk of mortality. Coronary angiogram (56.5%) revealed single-vessel disease (45.8%) as the most common finding. Percutaneous coronary intervention was performed in 53 patients (36%), at a median of 36 h (interquartile range 30-72) after symptom onset.
Patients with a delayed presentation after CS-STEMI were younger and more likely to have single-vessel disease. We found a high in-hospital mortality of 42.9%. Appropriate randomized studies are required to evaluate the optimal treatment strategies in these patients.
ST段抬高型心肌梗死(STEMI)后延迟就诊且并发心源性休克(CS-STEMI)在发展中国家较为常见,由于血运重建延迟导致大量心肌梗死,这是一种具有挑战性的情况。我们旨在评估CS-STEMI后延迟就诊患者的临床特征、血管造影特征及预后预测因素。
在一家三级转诊中心前瞻性招募了147例症状发作后至接受适当医疗护理时间≥12小时的CS-STEMI患者。
接受适当护理的中位时间为24小时(四分位间距18 - 48小时)。平均年龄为58.7±11.1岁。左心室泵衰竭是休克的主要原因(67.3%),而机械并发症占病例的14.9%,右心室梗死占13.6%。总体住院死亡率为42.9%。急性肾损伤[比值比(OR)8.04;95%置信区间(CI)3.08 - 20.92]、室性心动过速(OR 7.04;CI 2.09 - 23.63)、机械并发症(OR 6.46;CI 1.80 - 23.13)和前壁梗死(OR 3.18;CI 1.01 - 9.97)与死亡风险增加独立相关。冠状动脉造影(56.5%)显示单支血管病变(45.8%)是最常见的发现。53例患者(36%)接受了经皮冠状动脉介入治疗,症状发作后的中位时间为36小时(四分位间距30 - 72小时)。
CS-STEMI后延迟就诊的患者更年轻,且更可能患有单支血管病变。我们发现住院死亡率高达42.9%。需要进行适当的随机研究来评估这些患者的最佳治疗策略。