From the Division of Trauma and Emergency Surgery, Department of Surgery (D.M.B., T.R.J., S.S., M.D., R.B.J., C.Z., E.S., R.M.S., M.G.S., D.H.J., B.J.E., S.E.N.), Greehey Children's Cancer Research Institute (Z.L.), and Department of Molecular Medicine (Z.L.), UT Health San Antonio, San Antonio, Texas; Department of Medicine, Uniformed Services University of the Health Sciences (D.M.B), Bethesda, MD and US Army Institute of Surgical Research (D.M.B., S.E.N.), Fort Sam Houston, Texas.
J Trauma Acute Care Surg. 2020 May;88(5):579-587. doi: 10.1097/TA.0000000000002612.
Traumatic injury can lead to a compromised intestinal epithelial barrier, decreased gut perfusion, and inflammation. While recent studies indicate that the gut microbiome (GM) is altered early following traumatic injury, the impact of GM changes on clinical outcomes remains unknown. Our objective of this follow-up study was to determine if the GM is associated with clinical outcomes in critically injured patients.
We conducted a prospective, observational study in adult patients (N = 67) sustaining severe injury admitted to a level I trauma center. Fecal specimens were collected on admission to the emergency department, and microbial DNA from all samples was analyzed using the Quantitative Insights Into Microbial Ecology pipeline and compared against the Greengenes database. α-Diversity and β-diversity were estimated using the observed species metrics and analyzed with t tests and permutational analysis of variance for overall significance, with post hoc pairwise analyses.
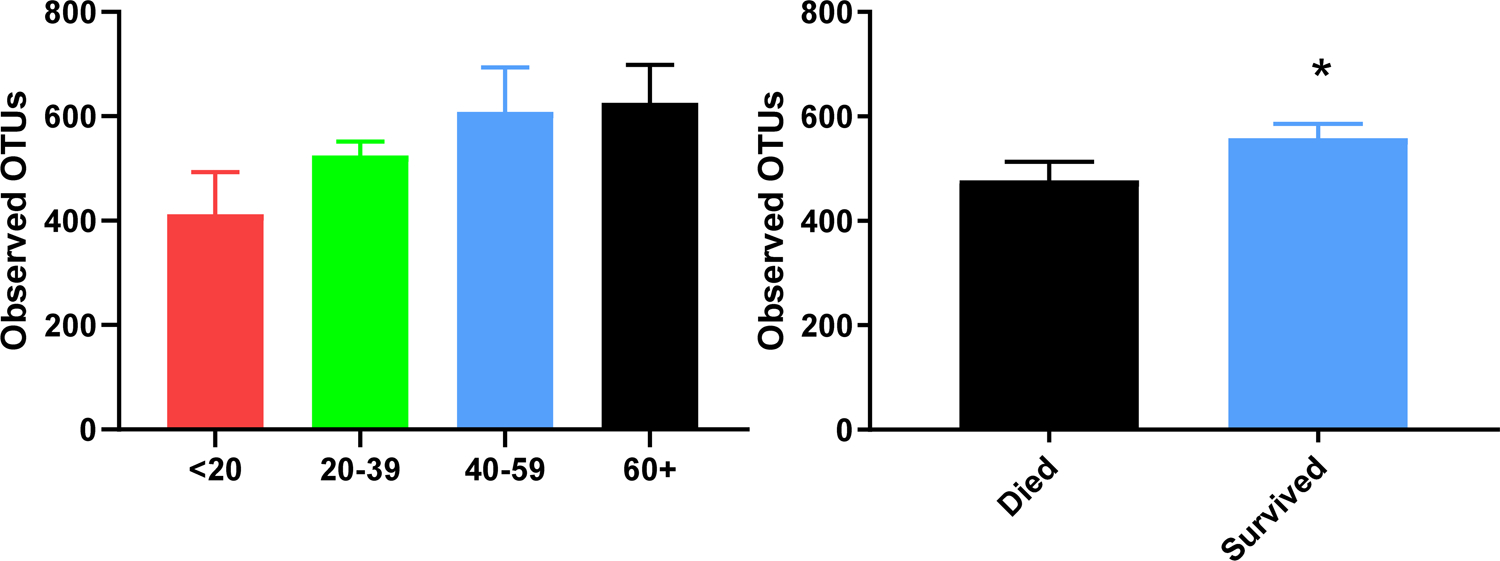
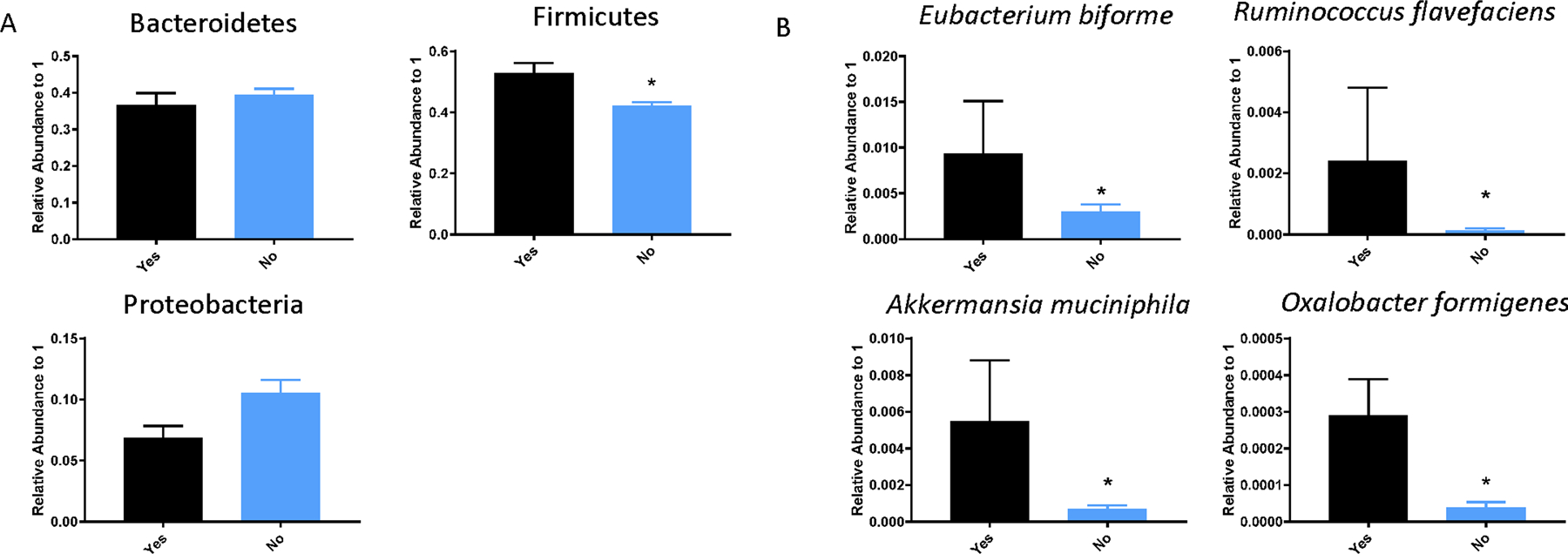
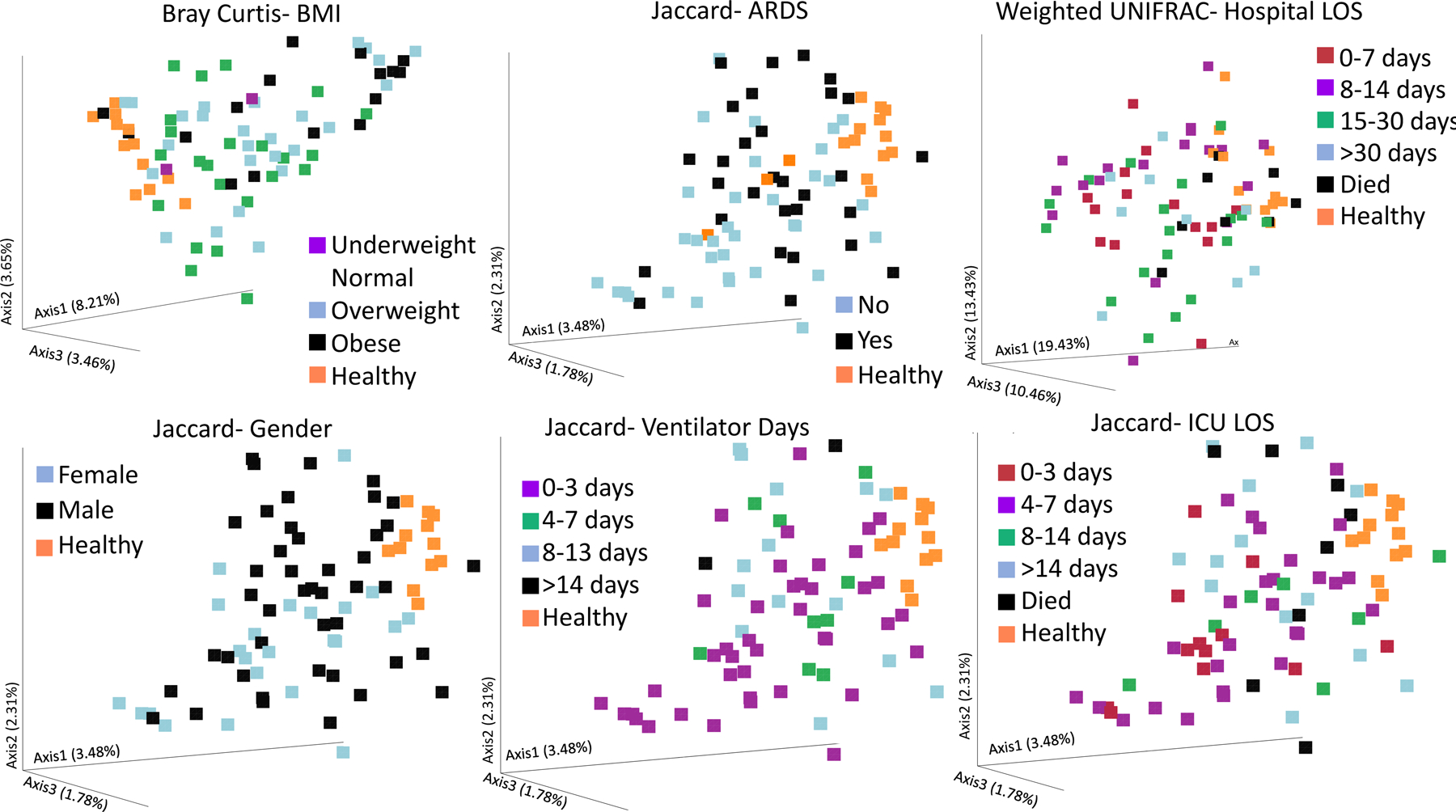
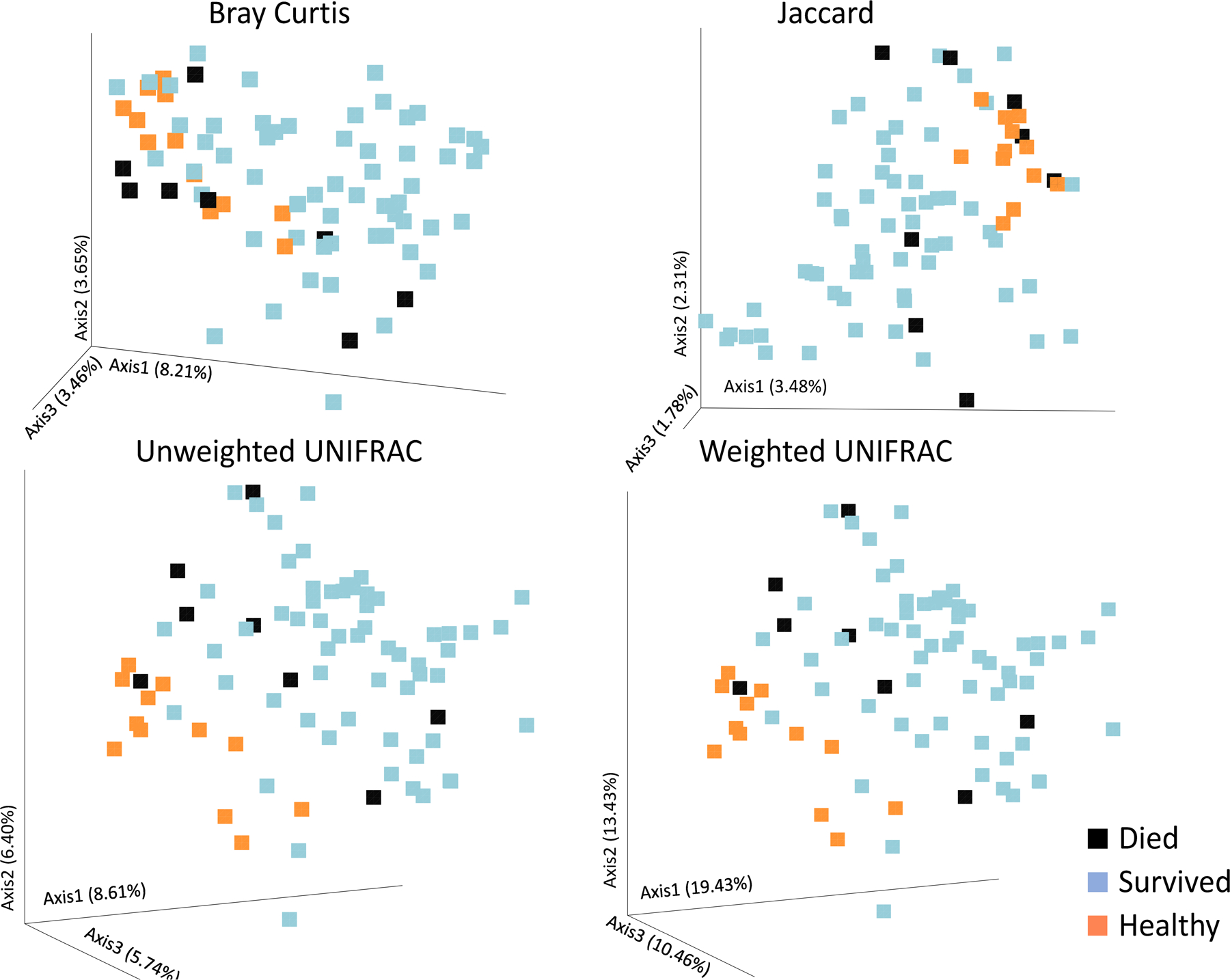
Our patient population consisted of 63% males with a mean age of 44 years. Seventy-eight percent of the patients suffered blunt trauma with 22% undergoing penetrating injuries. The mean body mass index was 26.9 kg/m. Significant differences in admission β-diversity were noted by hospital length of stay, intensive care unit hospital length of stay, number of days on the ventilator, infections, and acute respiratory distress syndrome (p < 0.05). β-Diversity on admission differed in patients who died compared with patients who lived (mean time to death, 8 days). There were also significantly less operational taxonomic units in samples from patients who died versus those who survived. A number of species were enriched in the GM of injured patients who died, which included some traditionally probiotic species such as Akkermansia muciniphilia, Oxalobacter formigenes, and Eubacterium biforme (p < 0.05).
Gut microbiome diversity on admission in severely injured patients is predictive of a variety of clinically important outcomes. While our study does not address causality, the GM of trauma patients may provide valuable diagnostic and therapeutic targets for the care of injured patients.
Prognostic and epidemiological, level III.
创伤可导致肠上皮屏障受损、肠道灌注减少和炎症。虽然最近的研究表明,创伤后早期肠道微生物组(GM)发生改变,但 GM 变化对临床结果的影响尚不清楚。本研究的目的是确定 GM 是否与重症创伤患者的临床结果相关。
我们对入住一级创伤中心的成年严重创伤患者(N=67)进行了前瞻性观察性研究。在急诊科就诊时采集粪便标本,使用定量微生物生态分析(QIIME)管道对所有样本的微生物 DNA 进行分析,并与 Greengenes 数据库进行比较。使用观察到的物种指标估计 α 多样性和 β 多样性,并使用 t 检验和方差分析进行整体显著性分析,并用事后两两分析进行检验。
我们的患者人群中男性占 63%,平均年龄为 44 岁。78%的患者为钝性创伤,22%为穿透性损伤。平均 BMI 为 26.9kg/m。住院时间、重症监护病房住院时间、呼吸机使用天数、感染和急性呼吸窘迫综合征的住院患者的β 多样性存在显著差异(p<0.05)。与存活患者相比,死亡患者的入院β 多样性存在显著差异(平均死亡时间为 8 天)。死亡患者样本中的操作分类单位也明显少于存活患者。死亡患者的 GM 中存在大量丰富的物种,包括一些传统的益生菌,如阿克曼氏菌(Akkermansia muciniphilia)、产草酸杆菌(Oxalobacter formigenes)和双歧杆菌(Eubacterium biforme)(p<0.05)。
严重创伤患者入院时 GM 多样性可预测多种临床重要结局。虽然本研究未探讨因果关系,但创伤患者的 GM 可能为创伤患者的治疗提供有价值的诊断和治疗靶点。
预后和流行病学,III 级。