Yeom Seung-Seop, Lee Soo Young, Kwak Han Deok, Kim Chang Hyun, Kim Young Jin, Kim Hyeong Rok
Department of Surgery, Chonnam National University Hwasun Hospital and Medical School, Hwasun, South Korea.
Medicine (Baltimore). 2020 Feb;99(7):e19258. doi: 10.1097/MD.0000000000019258.
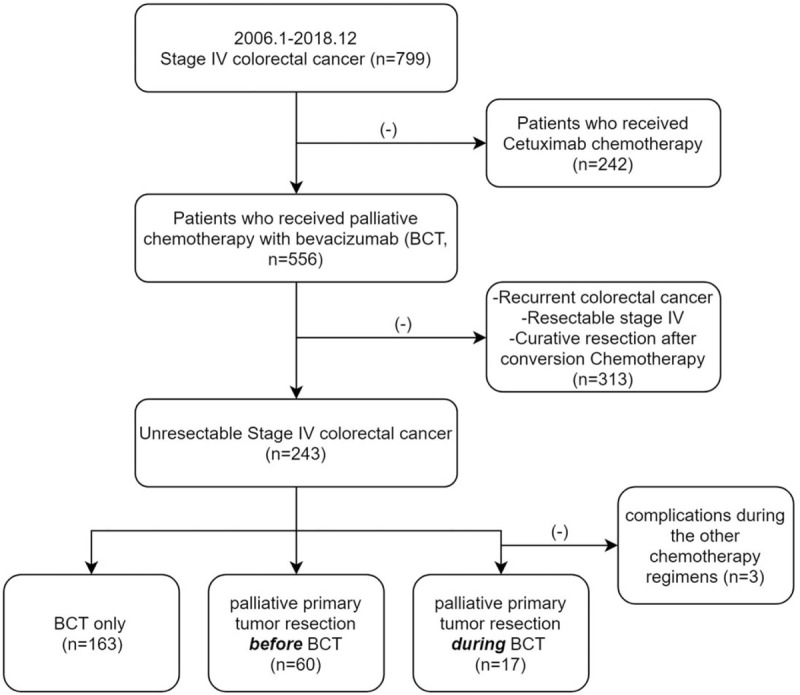
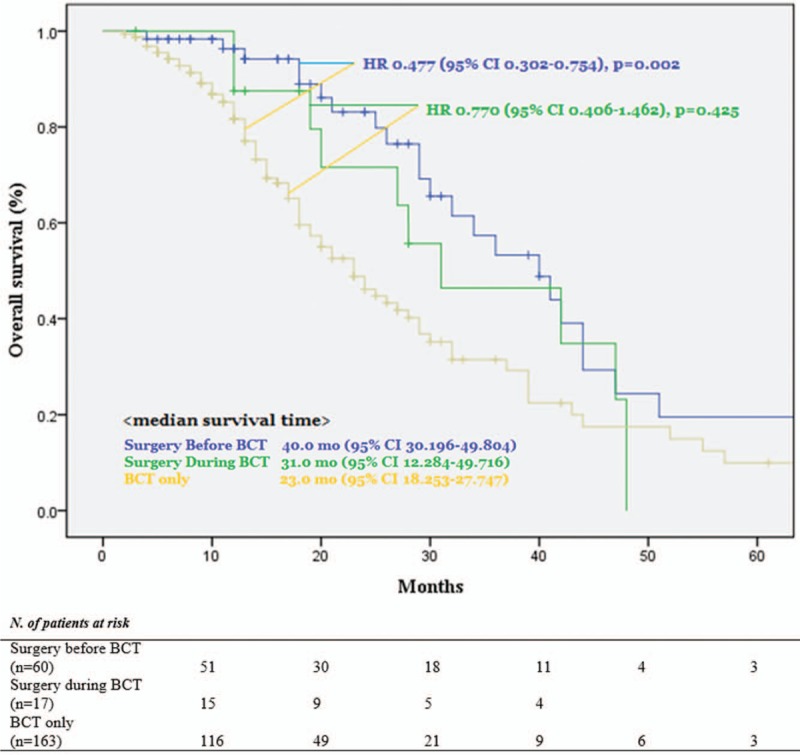
Primary tumor resection (PTR) for unresectable metastatic colorectal cancer (mCRC) patients has been documented to be associated with postoperative hyper-neovascularization and enhanced growth of metastases, which may be prevented by bevacizumab. This study aimed to investigate the survival outcome of PTR in patients who received palliative bevacizumab-containing chemotherapy (BCT).From January 2006 to December 2018, medical records of 240 mCRC patients who received palliative BCT at a single tertiary colorectal cancer center were retrospectively reviewed. Patients were classified into three groups: PTR-a (PTR before BCT, n = 60), PTR-b (PTR during BCT, n = 17), and BCT-only group (n = 163). Resectable mCRCs or recurrent diseases were excluded, and the end-point was overall survival (OS) rate.Three groups had similar age, cell differentiation, location of the primary tumor, and the number of metastatic organs. More than two-thirds of patients who received PTR experienced disease-progressions (PD) during their postoperative chemotherapy-free time (PTR-a vs PTR-b; 66.7% vs 76.5%, P = .170), but OS was not inferior to the BCT-only group (PTR-a vs BCT-only; HR 0.477 [95% CI 0.302-0.754], P = .002/PTR-b vs BCT-only; HR 0.77 [95% CI 0.406-1.462], P = .425). The postoperative chemotherapy-free time was similar between PTR-a and PTR-b (median 32.0 [14-98] days vs 41.0 [18-71] days, P = .142), but non-obstructive indications (perforation, bleeding, pain) were the more frequent in the PTR-b than PTR-a. Young age, the number of BCT, and PTR-a were the independent factors for OS.The efficacy of the PTR for unresectable mCRC has been controversial, but this study demonstrated that PTR should be considered for the unresectable mCRC patients regardless before and during BCT.
对于不可切除的转移性结直肠癌(mCRC)患者,原发肿瘤切除术(PTR)已被证明与术后高新生血管形成及转移灶生长增强有关,而贝伐单抗可能会预防这种情况。本研究旨在调查接受含贝伐单抗姑息化疗(BCT)的患者行PTR后的生存结局。
2006年1月至2018年12月,对一家三级结直肠癌中心接受姑息性BCT的240例mCRC患者的病历进行回顾性分析。患者分为三组:PTR-a组(BCT前PTR,n = 60)、PTR-b组(BCT期间PTR,n = 17)和单纯BCT组(n = 163)。排除可切除的mCRC或复发病例,终点为总生存率(OS)。
三组在年龄、细胞分化、原发肿瘤位置和转移器官数量方面相似。接受PTR的患者中超过三分之二在术后无化疗期间出现疾病进展(PTR-a组与PTR-b组;66.7%对76.5%,P = 0.170),但OS不低于单纯BCT组(PTR-a组与单纯BCT组;HR 0.477 [95%CI 0.302 - 0.754],P = 0.002/PTR-b组与单纯BCT组;HR 0.77 [95%CI 0.406 - 1.462],P = 0.425)。PTR-a组和PTR-b组的术后无化疗时间相似(中位数32.0 [14 - 98]天对41.0 [18 - 71]天,P = 0.142),但PTR-b组非梗阻性指征(穿孔、出血、疼痛)比PTR-a组更常见。年轻、BCT次数和PTR-a是OS的独立影响因素。
PTR对不可切除mCRC的疗效一直存在争议,但本研究表明,无论在BCT之前还是期间,对于不可切除的mCRC患者都应考虑行PTR。