Department of General, Visceral und Transplantation Surgery, Hospital of the Ludwig-Maximilian-University Munich, Munich, Germany.
Austrian Institute of Technology GmbH (AIT), Giefinggasse, Wien, Austria.
PLoS One. 2020 Feb 12;15(2):e0228615. doi: 10.1371/journal.pone.0228615. eCollection 2020.
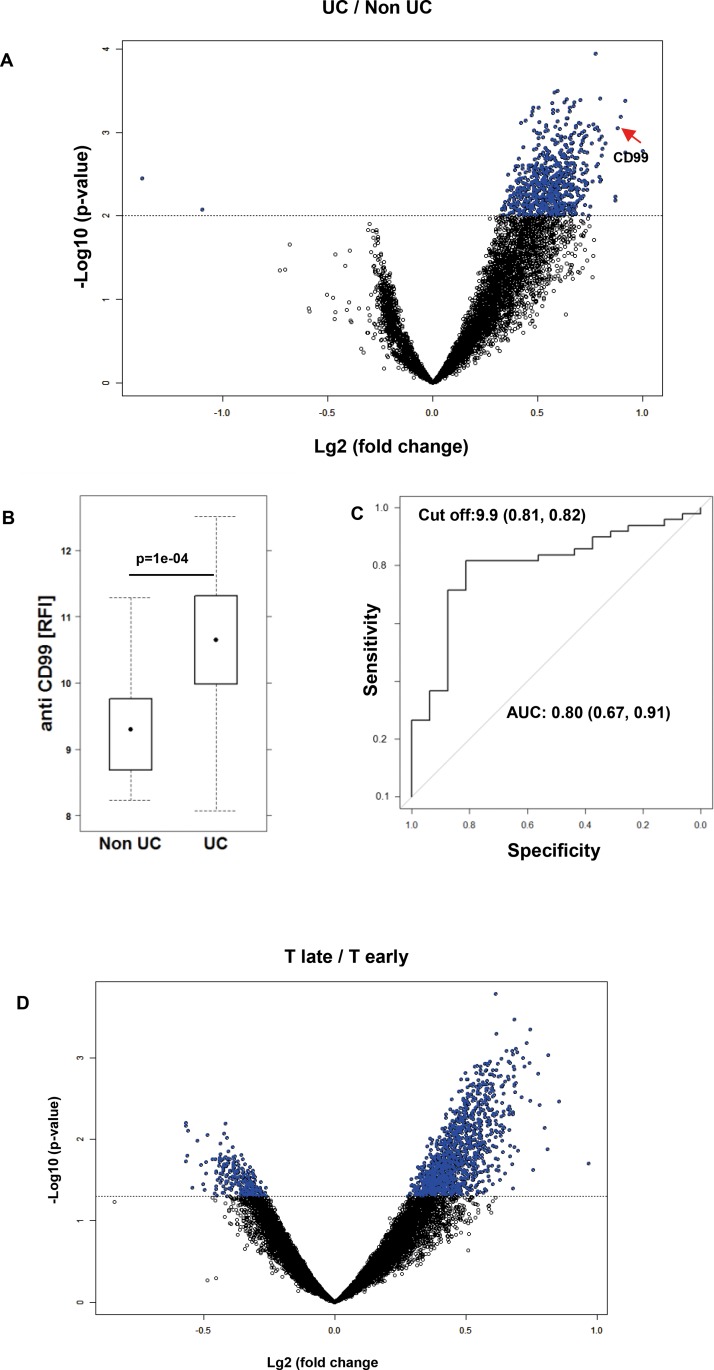
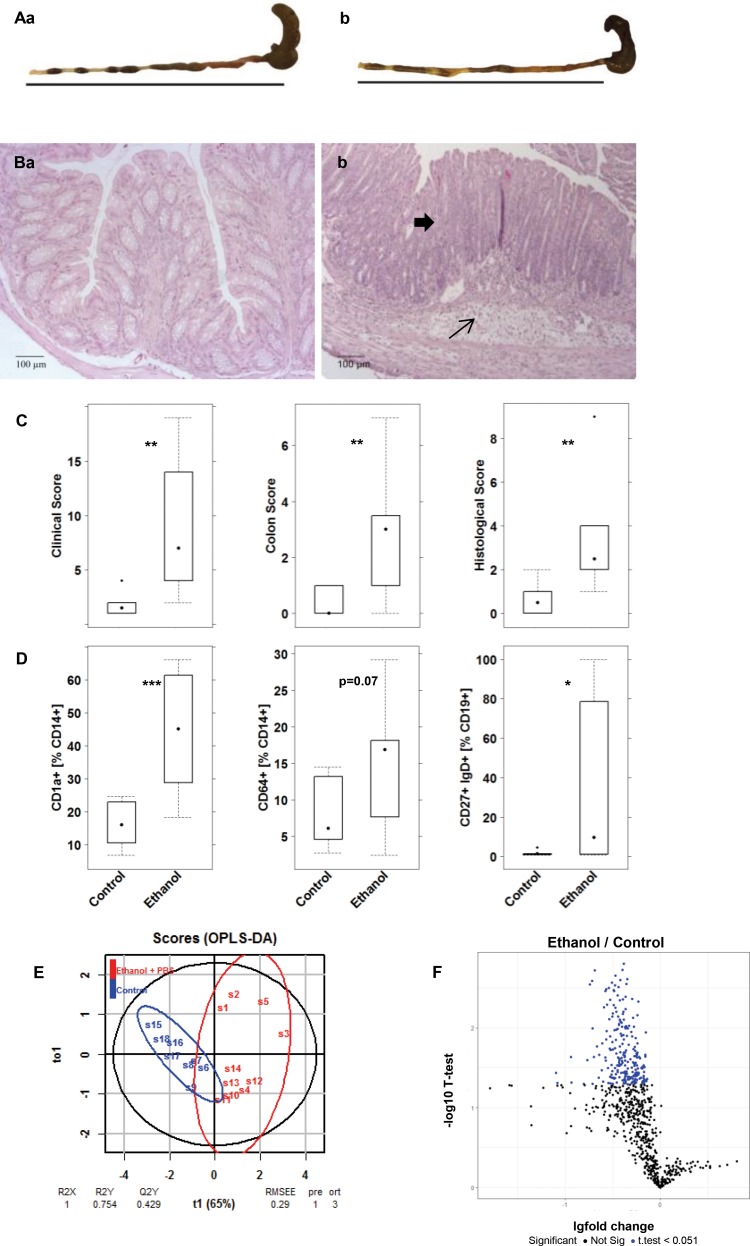
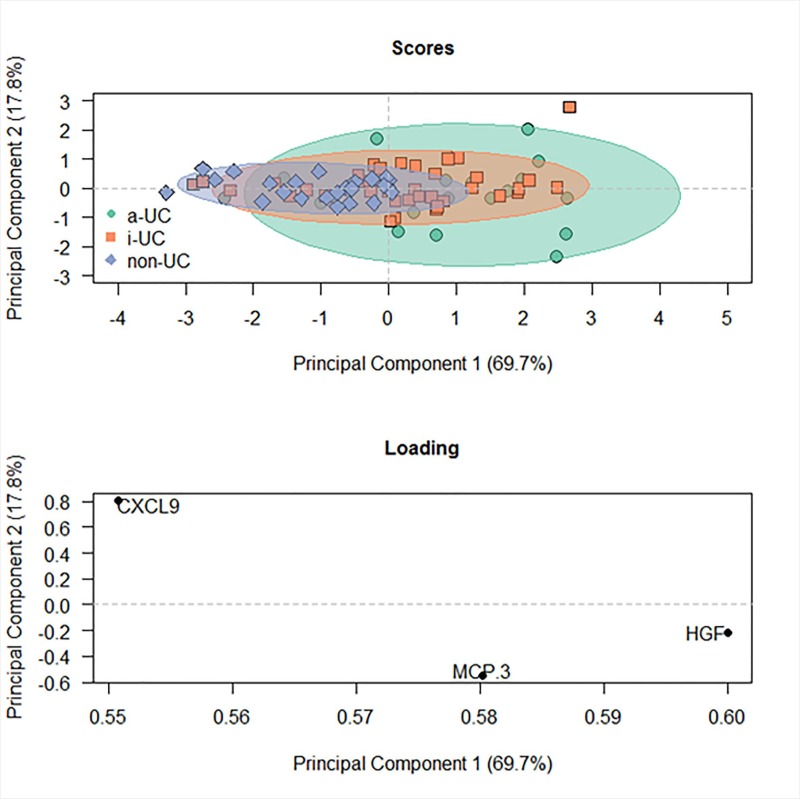
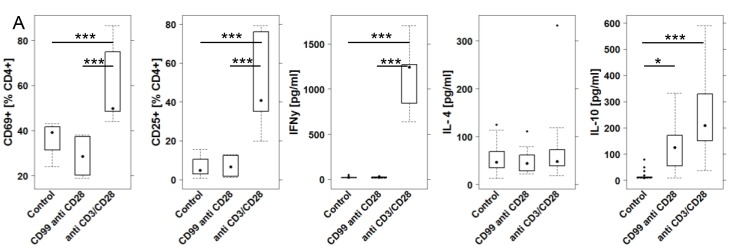
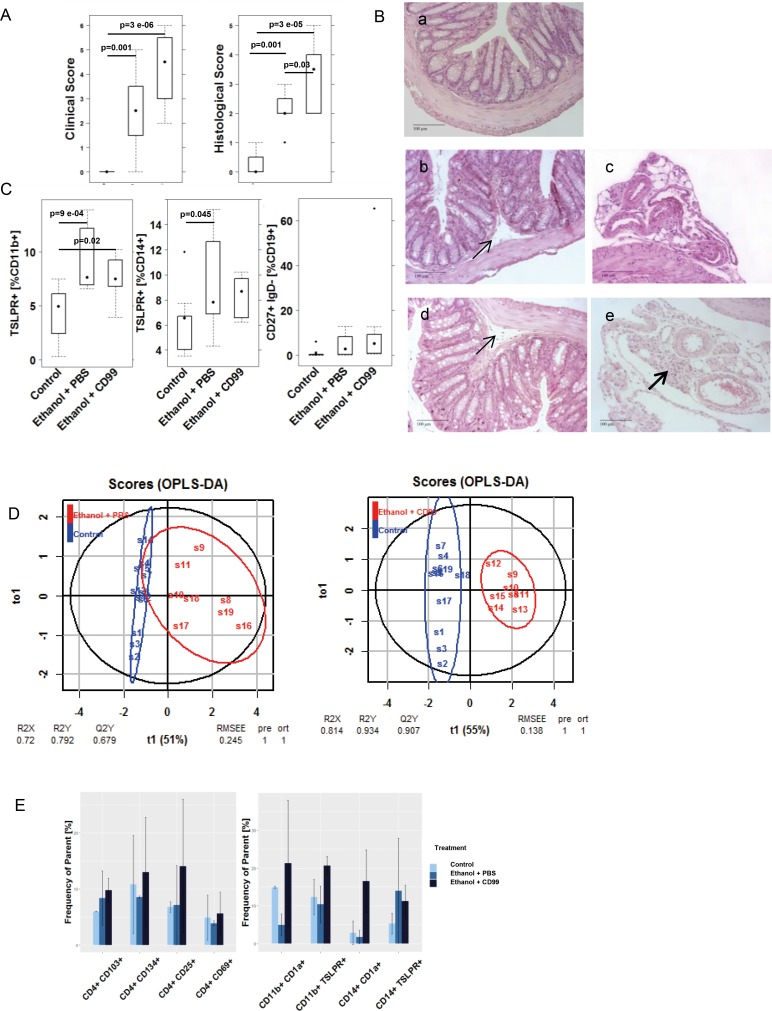
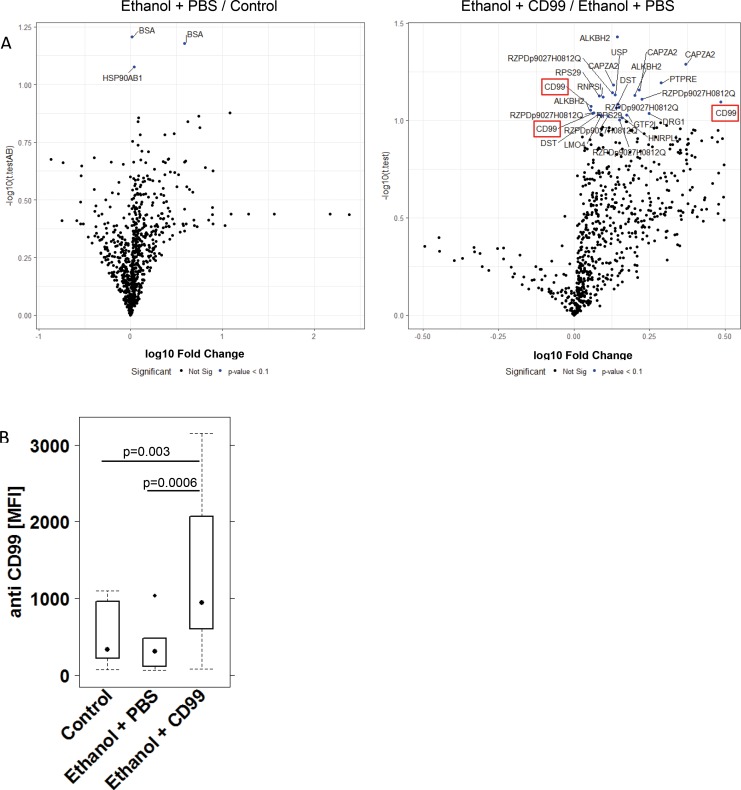
To date, no comprehensive analysis of autoantibodies in sera of patients with ulcerative colitis has been conducted. To analyze the spectrum of autoantibodies and to elucidate their role serum-IgG from UC patients (n = 49) and non-UC donors (n = 23) were screened by using a human protein microarray. Screening yielded a remarkable number of 697 differentially-reactive at the nominal 0·01 significance level (FDR<0·1) of the univariate test between the UC and the non-UC group. CD99 emerged as a biomarker to discriminate between both groups (p = 1e-04, AUC = 0·8). In addition, cytokines, chemokines and growth factors were analyzed by Olink's Proseek® Multiplex Inflammation-I 96×96 immuno-qPCR assay and 31 genes were significant at the nominal 0.05 level of the univariate test to discriminate between UC and non-UC donors. MCP-3, HGF and CXCL-9 were identified as the most significant markers to discriminate between UC patients with clinically active and inactive disease. Levels of CXCL10 (cor = 0.3; p = 0.02), CCL25 (cor = 0.25; p = 0.04) and CCL28 (cor = 0.3; p = 0.02) correlated positively with levels of anti CD99. To assess whether autoantibodies are detectable prior to diagnosis with UC, sera from nine donors at two different time points (T-early, median 21 months and T-late, median 6 months) were analyzed. 1201 features were identified with higher reactivity in samples at time points closer to clinical UC presentation. In vitro, additional challenge of peripheral mononuclear cells with CD99 did not activate CD4+ T cells but induced the secretion of IL-10 (-CD99: 20.21±20.25; +CD99: 130.20±89.55; mean ±sd; p = 0.015). To examine the effect of CD99 in vivo, inflammation and autoantibody levels were examined in NOD/ScidIL2Rγnull mice reconstituted with PBMC from UC donors (NSG-UC). Additional challenge with CD99 aggravated disease symptoms and pathological phenotype as indicated by the elevated clinical score (-CD99: 1·85 ± 1·94; +CD99: 4·25 ± 1·48) and histological score (-CD99: 2·16 ± 0·83; +CD99: 3·15 ± 1·16, p = 0·01). Furthermore, levels of anti-CD99 antibodies increased (Control: 398 ± 323; mean MFI ± sd; Ethanol + PBS: 358 ±316; Ethanol + CD99: 1363 ± 1336; Control versus Ethanol + CD99: p = 0.03). In a highly inflammatory environment, frequencies of pro-inflammatory M1 monocytes (CD14+ CD64+: unchallenged 8.09±4.72; challenged 14.2±8.62; p = 0.07; CD14+ CD1a+: unchallenged 16.29 ±6.97; challenged 43.81±14.4, p = 0.0003) increased and levels of autoantibodies in serum decreased in the NSG-UC mouse model. These results suggest that autoantibodies are potent biomarkers to discriminate between UC and non-UC and indicate risk to develop UC. In an inflammatory environment, auto-antibodies may promote the pathological phenotype by activating M1 monocytes in the NSG-UC animal model and also in patients with UC.
迄今为止,尚未对溃疡性结肠炎患者血清中的自身抗体进行全面分析。为了分析自身抗体的谱,并阐明其作用,我们使用人类蛋白质微阵列对 49 例溃疡性结肠炎患者(UC 组)和 23 例非 UC 供体(非 UC 组)的血清 IgG 进行了筛选。筛选产生了大量的差异反应,在 UC 组和非 UC 组之间,名义显著性水平为 0.01(FDR<0.1)的单变量检验中,有 697 个差异反应(p=1e-04,AUC=0.8)。CD99 作为区分两组的生物标志物(p=1e-04,AUC=0.8)。此外,还通过 Olink 的 Proseek® Multiplex Inflammation-I 96×96 immuno-qPCR assay 分析了细胞因子、趋化因子和生长因子,在 UC 组和非 UC 组之间,31 个基因在名义显著性水平为 0.05 的单变量检验中显著。MCP-3、HGF 和 CXCL-9 被鉴定为区分 UC 患者活动性和非活动性疾病的最显著标志物。CXCL10(cor=0.3;p=0.02)、CCL25(cor=0.25;p=0.04)和 CCL28(cor=0.3;p=0.02)的水平与抗 CD99 的水平呈正相关。为了评估自身抗体是否可以在 UC 诊断前检测到,我们分析了 9 名供体在两个不同时间点(早期 T,中位数 21 个月和晚期 T,中位数 6 个月)的血清。在更接近 UC 表现的时间点的样本中,鉴定出 1201 个具有更高反应性的特征。在体外,用 CD99 进一步刺激外周单核细胞不会激活 CD4+T 细胞,但会诱导 IL-10 的分泌(-CD99:20.21±20.25;+CD99:130.20±89.55;mean±sd;p=0.015)。为了研究 CD99 的作用,我们在接受 UC 供体 PBMC 重建的 NOD/ScidIL2Rγnull 小鼠中检查了炎症和自身抗体水平(NSG-UC)。用 CD99 进一步刺激加重了疾病症状和病理表型,临床评分升高(-CD99:1.85±1.94;+CD99:4.25±1.48),组织学评分升高(-CD99:2.16±0.83;+CD99:3.15±1.16,p=0.01)。此外,抗-CD99 抗体水平升高(对照:398±323;平均 MFI±sd;乙醇+PBS:358±316;乙醇+CD99:1363±1336;对照与乙醇+CD99 相比:p=0.03)。在高度炎症的环境中,促炎 M1 单核细胞的频率增加(CD14+CD64+:未刺激 8.09±4.72;刺激 14.2±8.62;p=0.07;CD14+CD1a+:未刺激 16.29±6.97;刺激 43.81±14.4,p=0.0003),血清中的自身抗体水平在 NSG-UC 小鼠模型中降低。这些结果表明,自身抗体是区分 UC 和非 UC 的有效生物标志物,并表明存在发生 UC 的风险。在炎症环境中,自身抗体可能通过激活 NSG-UC 动物模型和 UC 患者中的 M1 单核细胞来促进病理表型。