University of Chicago, Chicago, IL, USA.
Mayo Clinic, Rochester, MN, USA.
Mod Pathol. 2020 Jul;33(7):1410-1419. doi: 10.1038/s41379-020-0492-5. Epub 2020 Feb 12.
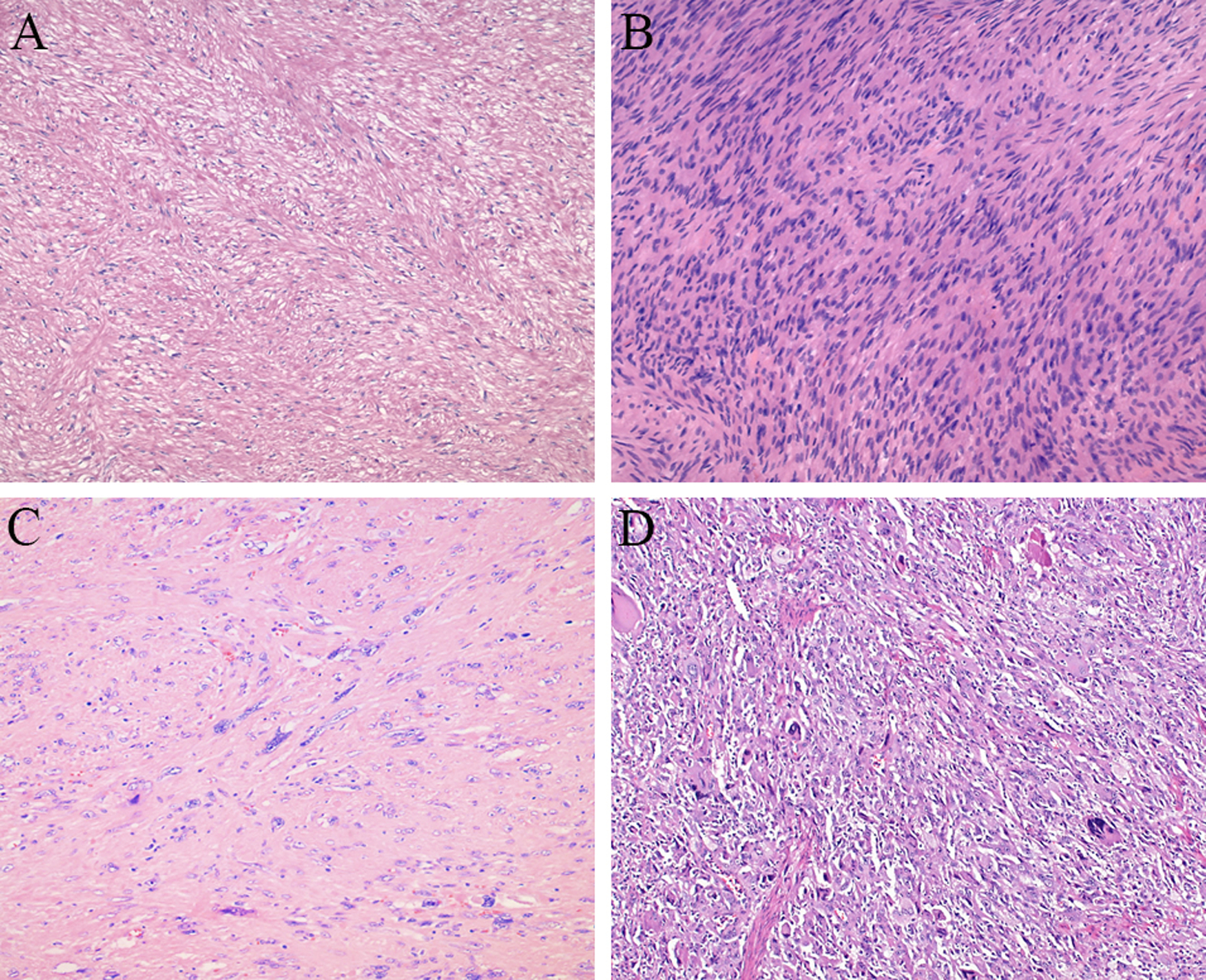
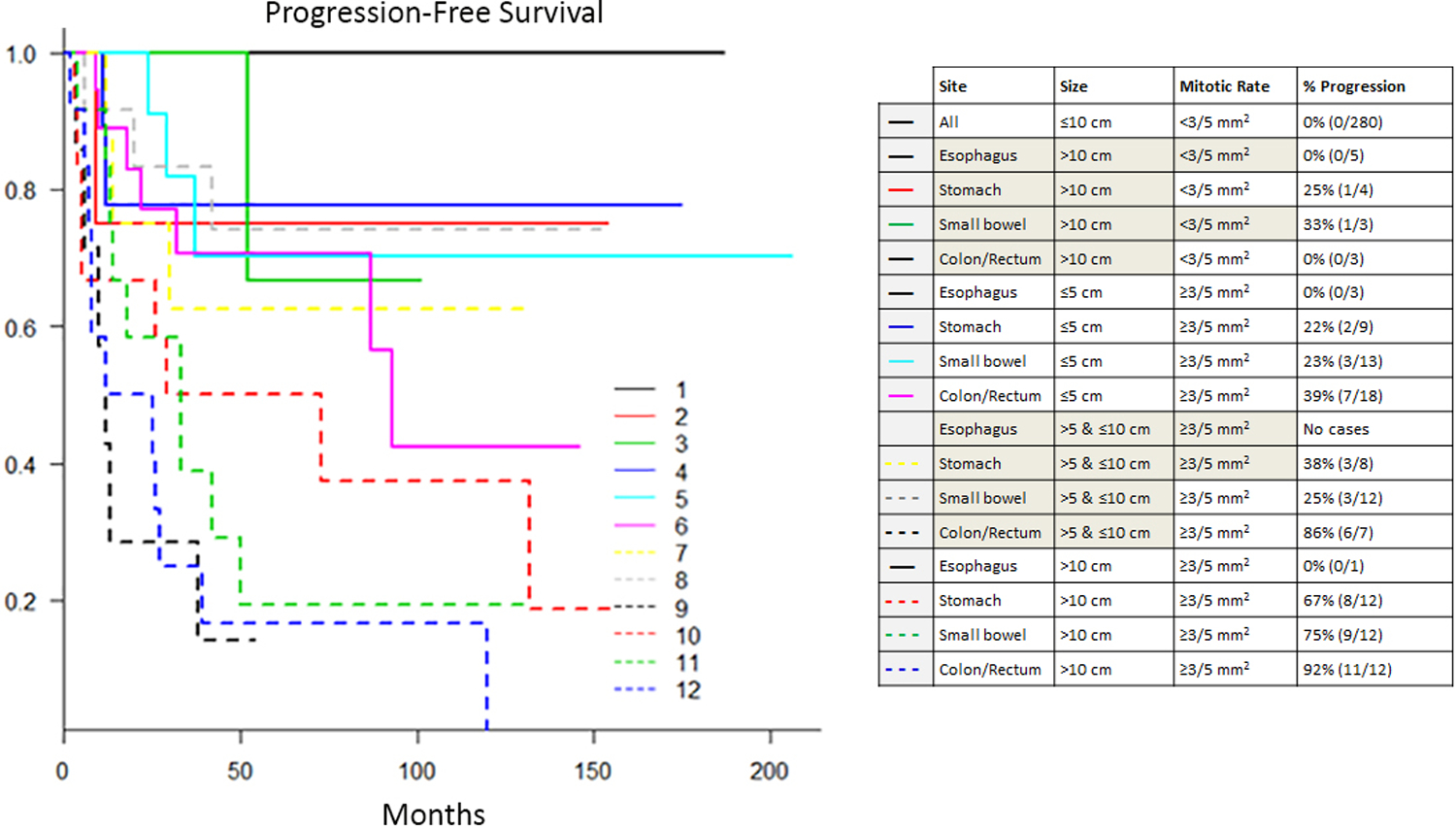
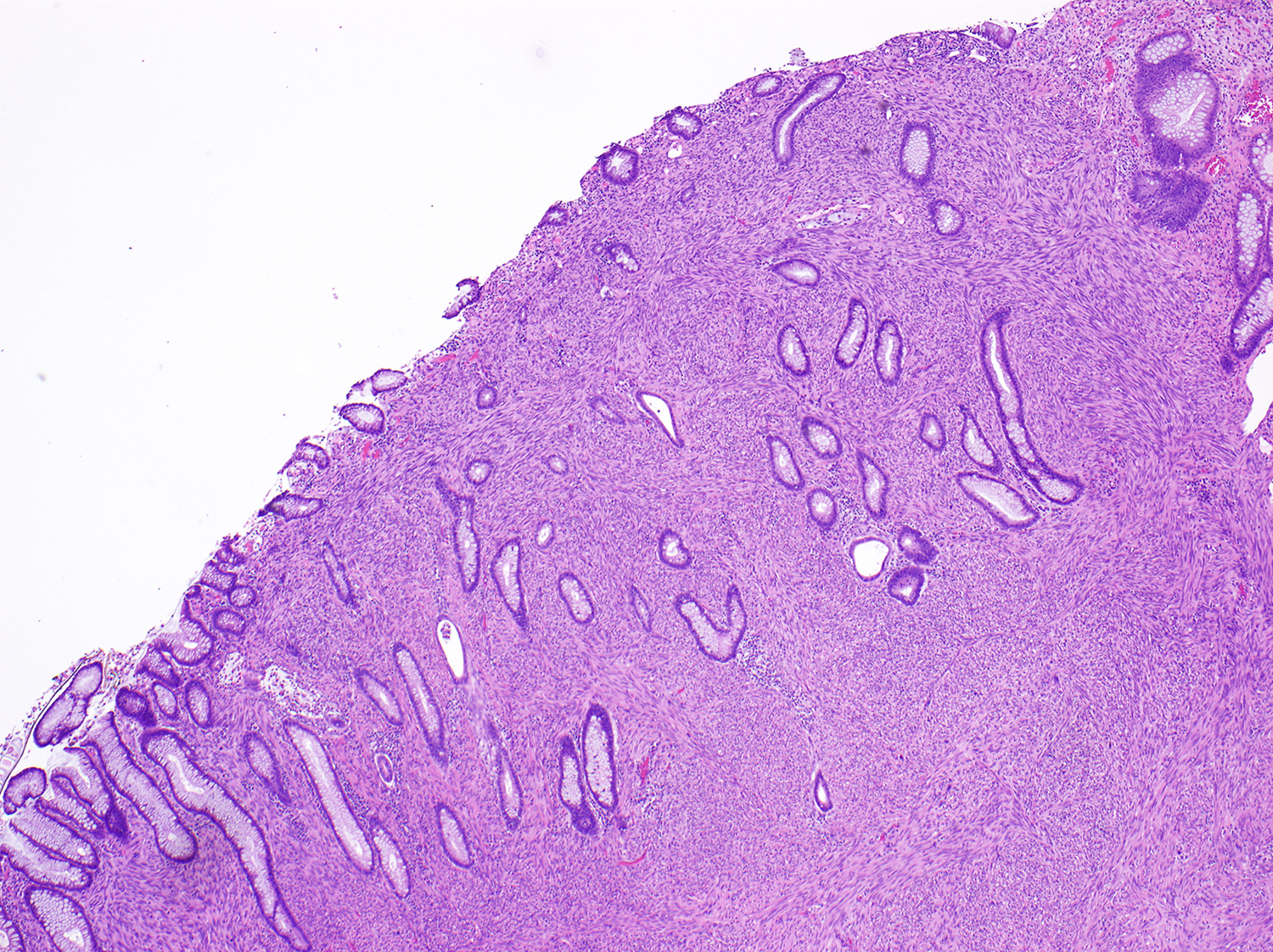
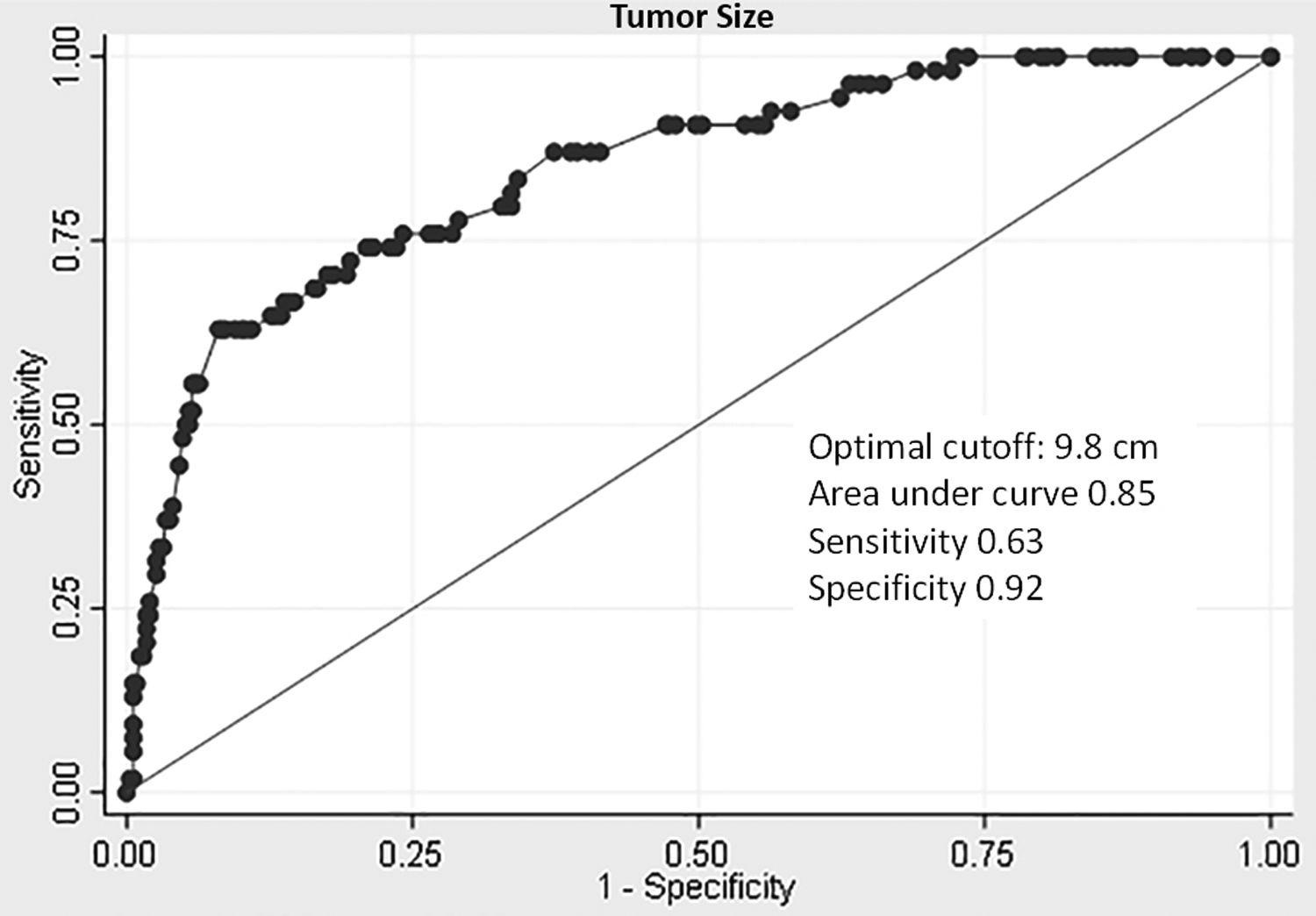
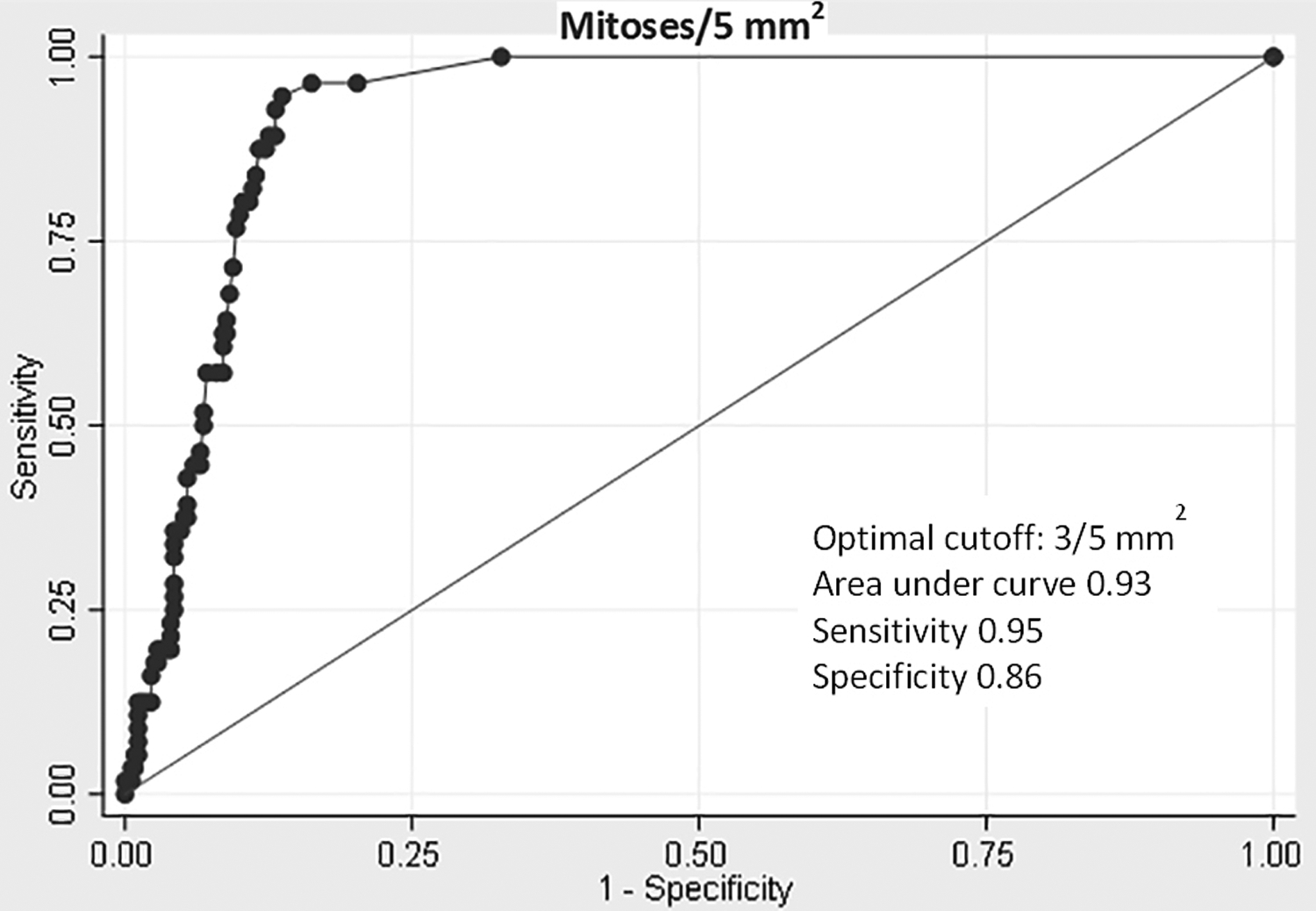
Smooth muscle tumors represent the second most common mural mesenchymal neoplasm in the gastrointestinal tract, but established criteria for prognostic assessment of these tumors are lacking. A large cohort of surgically resected intramural gastrointestinal smooth muscle tumors from 31 institutions was analyzed to identify potential prognostic features. Pathologic features were assessed by expert gastrointestinal and/or soft tissue pathologists at each center. Immunohistochemical confirmation was required. A total of 407 cases from the esophagus (n = 97, 24%), stomach (n = 180, 44%), small bowel (n = 74, 18%), and colorectum (n = 56, 14%) were identified. Patients ranged in age from 19 to 92 years (mean 55 years), with a slight female predominance (57%). Mean tumor size was 5.4 cm, with the largest tumor measuring 29 cm. Disease progression following surgery, defined as local recurrence, metastasis, or disease-related death, occurred in 56 patients (14%). Colorectal tumors were most likely to progress, followed by small bowel and gastric tumors. None of the esophageal tumors in this series progressed. Receiver operator characteristic analysis identified optimal cutoffs of 9.8 cm and 3 mitoses/5 mm for discriminating between progressive and non-progressive tumors. Histologic features strongly associated with progression by univariate analysis included moderate-to-severe atypia, high cellularity, abnormal differentiation (defined as differentiation not closely resembling that of normal smooth muscle), tumor necrosis, mucosal ulceration, lamina propria involvement, and serosal involvement (P < 0.0001 for all features). Age, sex, and margin status were not significantly associated with progression (P = 0.23, 0.82, and 0.07, respectively). A risk assessment table was created based on tumor site, size, and mitotic count, and Kaplan-Meier plots of progression-free survival for each subgroup revealed progression-based tiers. Based on our findings, it appears that nonesophageal gastrointestinal smooth muscle tumors measuring >10 cm and/or showing ≥3 mitoses/5 mm may behave aggressively, and therefore close clinical follow-up is recommended in these cases.
平滑肌肿瘤是胃肠道第二常见的壁间间叶性肿瘤,但缺乏这些肿瘤的预后评估标准。对 31 个机构切除的肠壁间胃肠道平滑肌肿瘤进行了大规模队列分析,以确定潜在的预后特征。每个中心的胃肠和/或软组织病理专家评估了病理特征。需要免疫组织化学确认。从食管(n=97,24%)、胃(n=180,44%)、小肠(n=74,18%)和结直肠(n=56,14%)中确定了 407 例患者。患者年龄从 19 岁到 92 岁(平均 55 岁),女性略多(57%)。平均肿瘤大小为 5.4cm,最大肿瘤大小为 29cm。手术后疾病进展,定义为局部复发、转移或与疾病相关的死亡,发生在 56 例患者(14%)中。结直肠肿瘤最有可能进展,其次是小肠和胃肿瘤。本系列食管肿瘤无一例进展。受试者工作特征分析确定了 9.8cm 和 3 个有丝分裂/5mm 作为区分进展性和非进展性肿瘤的最佳临界值。单因素分析发现,与进展相关的组织学特征包括中重度异型性、高细胞性、异常分化(定义为分化与正常平滑肌差异较大)、肿瘤坏死、黏膜溃疡、固有层受累和浆膜受累(所有特征 P<0.0001)。年龄、性别和切缘状态与进展无显著相关性(P=0.23、0.82 和 0.07)。根据肿瘤部位、大小和有丝分裂计数制定了风险评估表,每个亚组的 Kaplan-Meier 无进展生存图显示了基于进展的分层。根据我们的发现,似乎非食管胃肠道平滑肌肿瘤>10cm 且/或有丝分裂数≥3 个/5mm 可能具有侵袭性,因此建议在这些情况下密切临床随访。