Department of Surgery, Division of Surgical Oncology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Department of Surgery, Division of Hepatopancreatobiliary Surgery and Liver Transplantation, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Ann Surg Oncol. 2020 Aug;27(8):2997-3008. doi: 10.1245/s10434-020-08237-8. Epub 2020 Feb 12.
The extent of surgery (ES) during cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS + HIPEC) is a well-known risk factor for major postoperative morbidity. Interestingly, the reliability of surgeons to predict the ES prior to CRS + HIPEC is unknown.
In this prospective, observational cohort study, five surgeons predicted the ES prior to surgery in all consecutive patients with peritoneal metastases (PM) who were scheduled for CRS + HIPEC between March 2018 and May 2019. After the preoperative work-up for CRS + HIPEC was completed, all surgeons independently predicted, for each individual patient, the resection or preservation of 22 different anatomical structures and the presence of a stoma post-HIPEC according to a standardized ES form. The actual ES during CRS + HIPEC was extracted from the surgical procedure report and compared with the predicted ES. Overall and individual positive (PPV) and negative predictive values (NPV) for each anatomical structure were calculated.
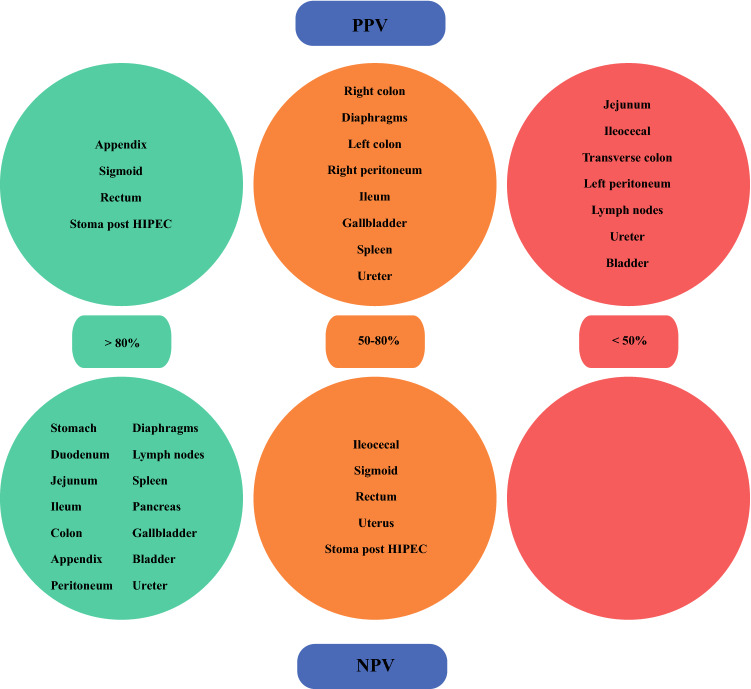
One hundred and thirty-one ES forms were collected from 32 patients who successfully underwent CRS + HIPEC. The number of resections was predicted correctly 24 times (18.3%), overestimated 57 times (43.5%), and underestimated 50 times (38.2%). Overall PPVs for the different anatomical structures ranged between 33.3 and 87.8%. Overall, NPVs ranged between 54.9 and 100%, and an NPV > 90% was observed for 12 anatomical structures.
Experienced surgeons seem to be able to better predict the anatomical structures that remain in situ after CRS + HIPEC, rather than predict the resections that were necessary to achieve a complete cytoreduction.
细胞减灭术联合腹腔内热灌注化疗(CRS+HIPEC)中的手术范围(ES)是术后发生重大并发症的一个众所周知的危险因素。有趣的是,外科医生在 CRS+HIPEC 术前预测 ES 的可靠性尚不清楚。
在这项前瞻性观察队列研究中,5 位外科医生在 2018 年 3 月至 2019 年 5 月期间对所有计划接受 CRS+HIPEC 的腹膜转移(PM)患者进行了术前评估,并对所有连续患者的 ES 进行了预测。在完成 CRS+HIPEC 的术前准备后,所有外科医生根据标准化 ES 表格,分别对每个患者独立预测了 22 个不同解剖结构的切除或保留情况,以及 HIPEC 术后造口的存在。从手术报告中提取 CRS+HIPEC 期间的实际 ES,并与预测 ES 进行比较。计算了每个解剖结构的总体和个体阳性预测值(PPV)和阴性预测值(NPV)。
从 32 例成功接受 CRS+HIPEC 的患者中收集了 131 份 ES 表。切除的数量预测正确 24 次(18.3%),高估 57 次(43.5%),低估 50 次(38.2%)。不同解剖结构的总体 PPV 范围在 33.3%至 87.8%之间。总体 NPV 范围在 54.9%至 100%之间,12 个解剖结构的 NPV 大于 90%。
经验丰富的外科医生似乎能够更好地预测 CRS+HIPEC 后仍保留在原位的解剖结构,而不是预测实现完全细胞减灭所需的切除。