From the Department of Anesthesiology and Perioperative Medicine (B.D.E., J.C.H., P.A.C., E.G., M.C.) Medicine Statistics Core (T.G.), University of California, Los Angeles, Los Angeles, California.
Anesthesiology. 2020 May;132(5):981-991. doi: 10.1097/ALN.0000000000003176.
Although clinical factors related to intraoperative opioid administration have been described, there is little research evaluating whether administration is influenced by drug formulation and, specifically, the unit dose of the drug. The authors hypothesized that the unit dose of hydromorphone is an independent determinant of the quantity of hydromorphone administered to patients intraoperatively.
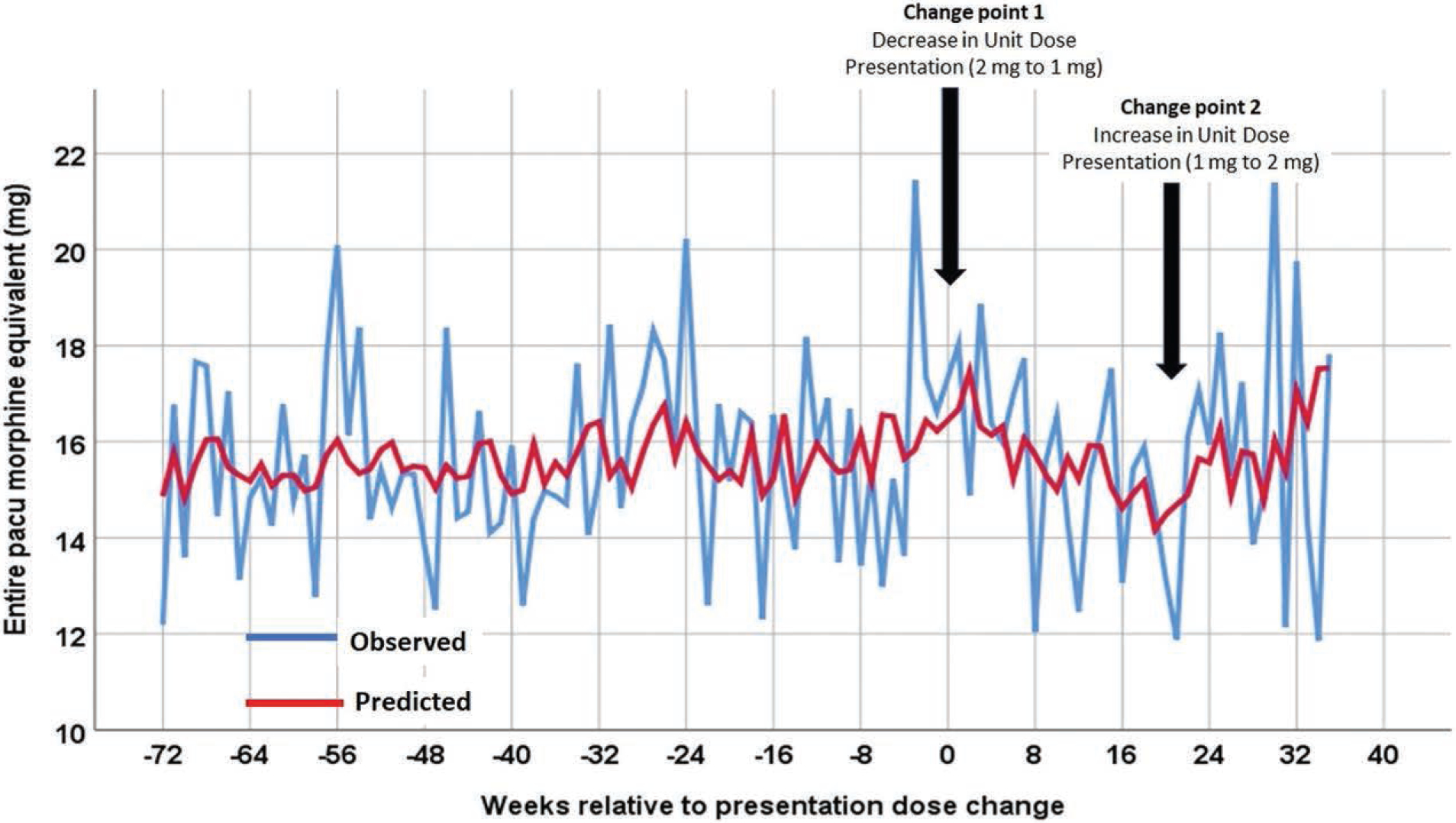
This observational cohort study included 15,010 patients who received intraoperative hydromorphone as part of an anesthetic at the University of California, Los Angeles hospitals from February 2016 to March 2018. Before July 2017, hydromorphone was available as a 2-mg unit dose. From July 1, 2017 to November 20, 2017, hydromorphone was only available in a 1-mg unit dose. On November 21, 2017, hydromorphone was reintroduced in the 2-mg unit dose. An interrupted time series analysis was performed using segmented Poisson regression with two change-points, the first representing the switch from a 2-mg to 1-mg unit dose, and the second representing the reintroduction of the 2-mg dose.
The 2-mg to 1-mg unit dose change was associated with a 49% relative decrease in the probability of receiving a hydromorphone dose greater than 1 mg (risk ratio, 0.51; 95% CI, 0.40-0.66; P < 0.0001). The reintroduction of a 2-mg unit dose was associated with a 48% relative increase in the probability of administering a dose greater than 1 mg (risk ratio, 1.48; 95% CI, 1.11-1.98; P = 0.008).
This observational study using an interrupted time series analysis demonstrates that unit dose of hydromorphone (2 mg vs. 1 mg) is an independent determinant of the quantity of hydromorphone administered to patients in the intraoperative period.
尽管已经描述了与术中阿片类药物给药相关的临床因素,但很少有研究评估给药是否受药物制剂影响,特别是药物的单位剂量影响。作者假设氢吗啡酮的单位剂量是术中给予患者氢吗啡酮量的独立决定因素。
这项观察性队列研究纳入了 2016 年 2 月至 2018 年 3 月期间在加利福尼亚大学洛杉矶分校医院接受术中氢吗啡酮麻醉的 15010 名患者。在 2017 年 7 月之前,氢吗啡酮的单位剂量为 2 毫克。从 2017 年 7 月 1 日至 2017 年 11 月 20 日,氢吗啡酮仅以 1 毫克的单位剂量供应。2017 年 11 月 21 日,重新引入 2 毫克单位剂量的氢吗啡酮。使用两段分段泊松回归进行中断时间序列分析,两个转折点分别代表从 2 毫克到 1 毫克单位剂量的转变,以及重新引入 2 毫克剂量的转折点。
从 2 毫克到 1 毫克单位剂量的变化与接受大于 1 毫克氢吗啡酮剂量的概率降低 49%(风险比,0.51;95%CI,0.40-0.66;P <0.0001)相关。重新引入 2 毫克单位剂量与给予大于 1 毫克剂量的概率增加 48%(风险比,1.48;95%CI,1.11-1.98;P = 0.008)相关。
这项使用中断时间序列分析的观察性研究表明,氢吗啡酮的单位剂量(2 毫克与 1 毫克)是术中给予患者氢吗啡酮量的独立决定因素。