Division of Sleep and Circadian Disorders, Departments of Medicine and Neurology, Brigham and Women's Hospital, Boston, Mass; Division of Sleep Medicine, Harvard Medical School, Boston, Mass.
Division of Sleep and Circadian Disorders, Departments of Medicine and Neurology, Brigham and Women's Hospital, Boston, Mass; Division of Sleep Medicine, Harvard Medical School, Boston, Mass; Department of Medicine, Division of General Pediatrics, Department of Medicine, Boston Children's Hospital, Boston, Mass.
Am J Med. 2020 Jul;133(7):e343-e354. doi: 10.1016/j.amjmed.2019.12.053. Epub 2020 Feb 13.
In 2011, the Accreditation Council for Graduate Medical Education (ACGME) instituted a 16-h limit on consecutive hours for first-year resident physicians. We sought to examine the effect of these work-hour regulations on physician safety.
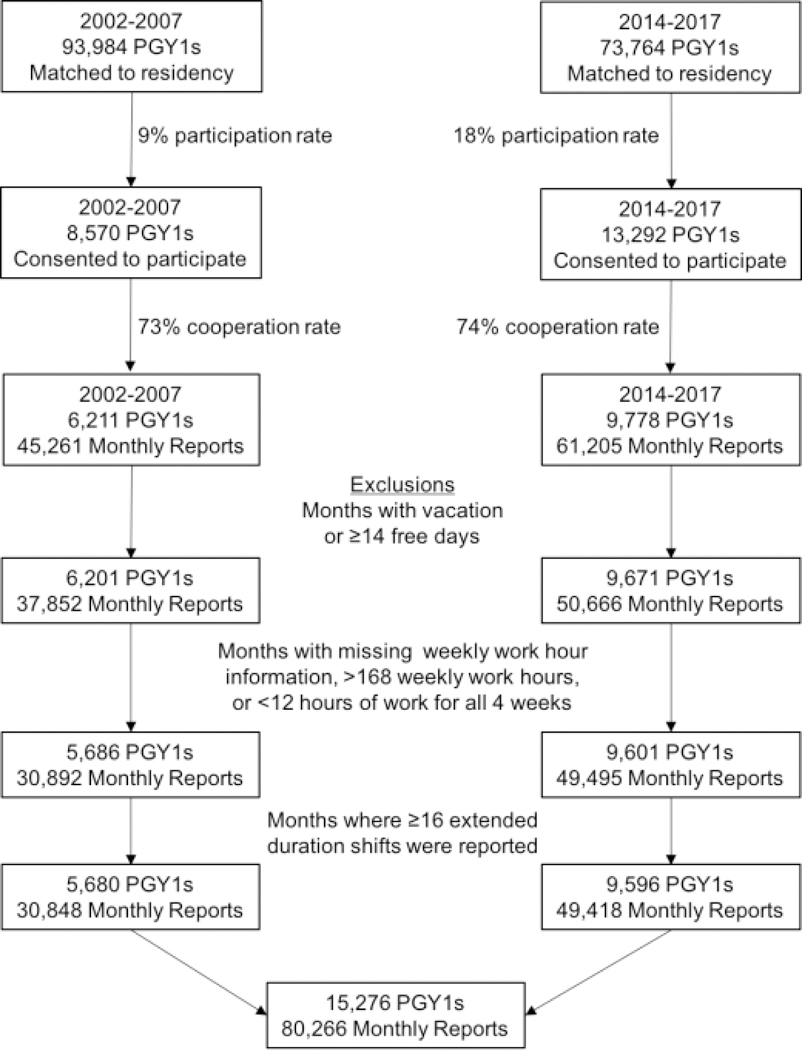
All medical students matched to a US residency program from 2002 to 2007 and 2014 to 2017 were invited to participate in prospective cohort studies. Each month participants reported hours of work, extended duration shifts, and adverse safety outcomes, including motor vehicle crashes, percutaneous injuries, and attentional failures. The incidence of each outcome was compared before and after the 2011 ACGME work-hour limit. Hypotheses were tested using generalized linear models adjusted for potential confounders.
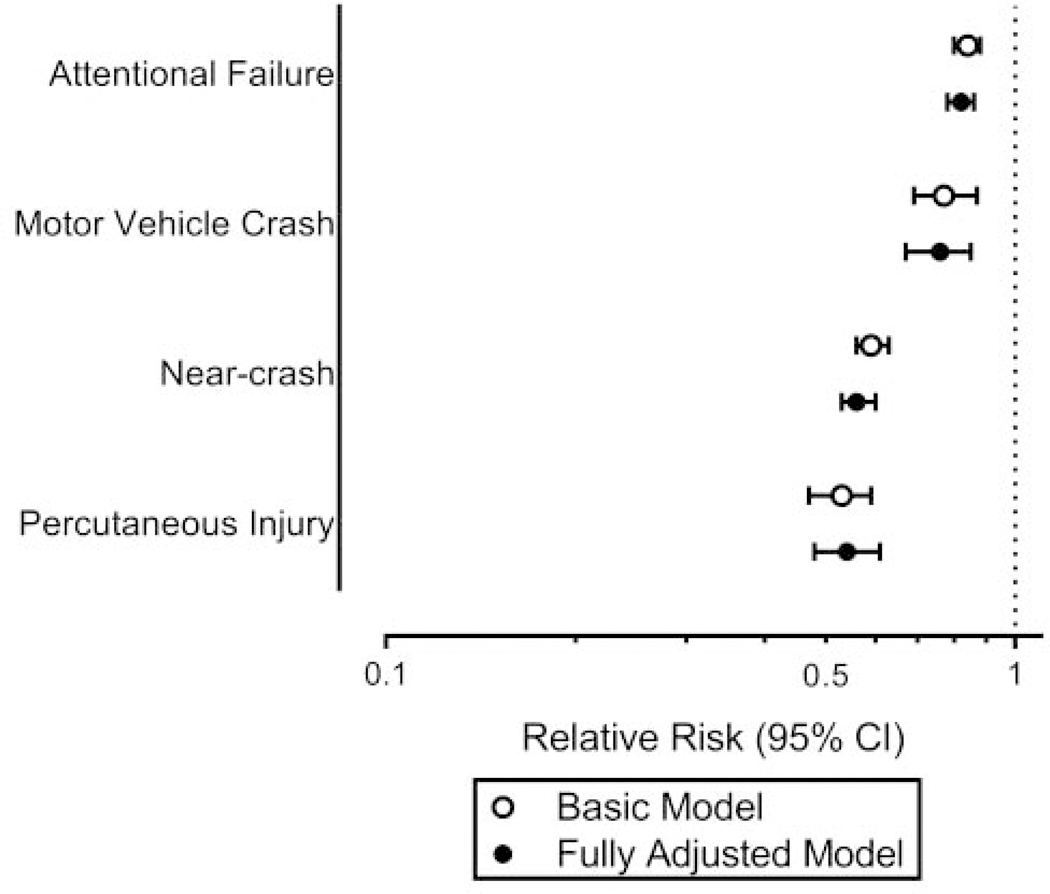
Of all first-year resident physicians nationwide, 13% participated in the study, with 80,266 monthly reports completed by 15,276 first-year resident physicians. Following implementation of the 16-h 2011 ACGME work-hour limit, the mean number of extended duration (≥24-h) shifts per month decreased from 3.9 to 0.2. The risk of motor vehicle crash decreased 24% (relative risk [RR] 0.76; 0.67-0.85), percutaneous injury risk decreased more than 40% (relative risk 0.54; 0.48-0.61), and the rate of attentional failures was reduced 18% (incidence rate ratio [IRR] 0.82; 0.78-0.86). Extended duration shifts and prolonged weekly work hours were associated with an increased risk of adverse safety outcomes independent of cohort.
The 2011 ACGME work-hour limit was associated with meaningful improvements in physician safety and health. Surveillance is needed to monitor the ongoing impact of work hours on physician safety, health, and well-being.
2011 年,美国毕业后医学教育认证委员会(ACGME)对住院医师实施了连续 16 小时工作时间限制。我们旨在研究这些工作时间规定对医生安全的影响。
所有在 2002 年至 2007 年和 2014 年至 2017 年期间与美国住院医师计划相匹配的医学生都被邀请参加前瞻性队列研究。每月,参与者报告工作时间、延长工作时间班次和不良安全结果,包括机动车事故、穿刺伤和注意力失败。在 2011 年 ACGME 工作时间限制之前和之后,比较每种结果的发生率。使用广义线性模型检验假设,该模型调整了潜在混杂因素。
在全国范围内,所有第一年住院医师中有 13%参与了这项研究,15276 名第一年住院医师完成了 80266 次月度报告。在 2011 年 ACGME 实施 16 小时工作时间限制后,每月延长工作时间(≥24 小时)班次的平均数量从 3.9 减少到 0.2。机动车事故的风险降低了 24%(相对风险 [RR] 0.76;0.67-0.85),穿刺伤风险降低了 40%以上(相对风险 0.54;0.48-0.61),注意力失败率降低了 18%(发病率比 [IRR] 0.82;0.78-0.86)。延长的工作时间班次和每周延长的工作时间与不良安全结果的风险增加有关,独立于队列。
2011 年 ACGME 的工作时间限制与医生安全和健康的显著改善有关。需要进行监测,以监测工作时间对医生安全、健康和福祉的持续影响。