U.S. Military HIV Research Program, Walter Reed Army Institute of Research, Silver Spring, MD, USA.
Henry M. Jackson Foundation for the Advancement of Military Medicine, Bethesda, MD, USA.
J Int AIDS Soc. 2020 Feb;23(2):e25446. doi: 10.1002/jia2.25446.
World Health Organization (WHO) guidelines have shifted over time to recommend earlier initiation of antiretroviral therapy (ART) and now encourage ART initiation on the day of HIV diagnosis, if possible. However, barriers to ART access may delay initiation in resource-limited settings. We characterized temporal trends and other factors influencing the interval between HIV diagnosis and ART initiation among participants enrolled in a clinic-based cohort across four African countries.
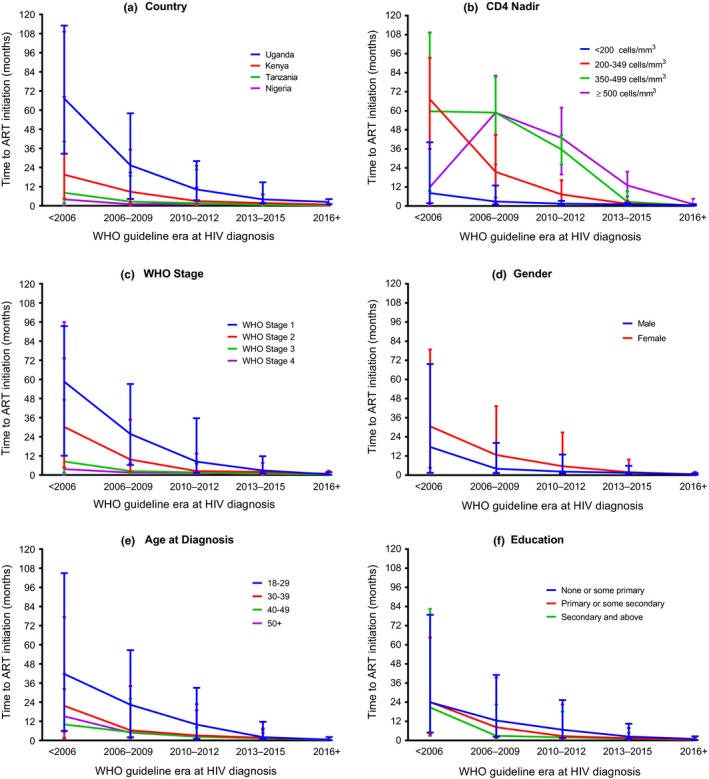
The African Cohort Study enrols adults engaged in care at 12 sites in Uganda, Kenya, Tanzania and Nigeria. Participants provide a medical history, complete a physical examination and undergo laboratory assessments every six months. Participants with recorded dates of HIV diagnosis were categorized by WHO guideline era (<2006, 2006 to 2009, 2010 to 2012, 2013 to 2015, ≥2016) at the time of diagnosis. Cox proportional hazard modelling was used to estimate hazard ratios (HRs) and 95% confidence intervals (95% CI) for time to ART initiation.
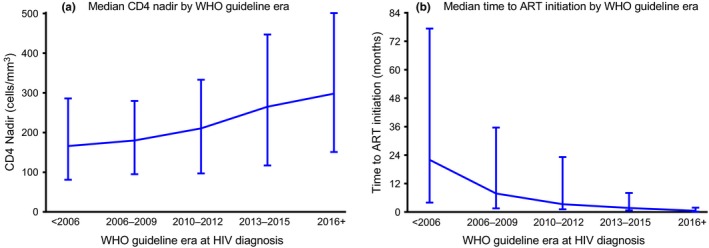
From January 2013 to September 2019, a total of 2888 adults living with HIV enrolled with known diagnosis dates. Median time to ART initiation decreased from 22.0 months (interquartile range (IQR) 4.0 to 77.3) among participants diagnosed prior to 2006 to 0.5 months (IQR 0.2 to 1.8) among those diagnosed in 2016 and later. Comparing those same periods, CD4 nadir increased from a median of 166 cells/mm (IQR: 81 to 286) to 298 cells/mm (IQR: 151 to 501). In the final adjusted model, participants diagnosed in each subsequent WHO guideline era had increased rates of ART initiation compared to those diagnosed before 2006. CD4 nadir ≥500 cells/mm was independently associated with a lower rate of ART initiation as compared to CD4 nadir <200 cells/mm (HR: 0.32; 95% CI: 0.28 to 0.37). Age >50 years at diagnosis was independently associated with shorter time to ART initiation as compared to 18 to 29 years (HR: 1.38; 95% CI: 1.19 to 1.61).
Consistent with changing guidelines, the interval between diagnosis and ART initiation has decreased over time. Still, many adults living with HIV initiated treatment with low CD4, highlighting the need to diagnose HIV earlier while improving access to immediate ART after diagnosis.
世界卫生组织(WHO)的指南随着时间的推移发生了变化,现在建议尽早开始抗逆转录病毒治疗(ART),并在可能的情况下在 HIV 诊断当天开始 ART。然而,在资源有限的情况下,获得 ART 的障碍可能会延迟开始治疗的时间。我们描述了在四个非洲国家的基于诊所的队列中参与者中 HIV 诊断和开始 ART 之间的时间间隔的时间趋势和其他影响因素。
非洲队列研究招募了在乌干达、肯尼亚、坦桑尼亚和尼日利亚的 12 个地点接受护理的成年人。参与者提供病史,每六个月进行一次体检和实验室评估。根据诊断时的 WHO 指南时代(<2006、2006 年至 2009 年、2010 年至 2012 年、2013 年至 2015 年、≥2016 年),将有记录 HIV 诊断日期的参与者进行分类。使用 Cox 比例风险模型估计开始 ART 的时间的风险比(HR)和 95%置信区间(95%CI)。
从 2013 年 1 月至 2019 年 9 月,共有 2888 名患有 HIV 的成年人参加了已知诊断日期的研究。与 2006 年之前诊断的参与者相比,2016 年及以后诊断的参与者的 ART 起始中位时间从 22.0 个月(四分位距(IQR)4.0 至 77.3)减少到 0.5 个月(IQR 0.2 至 1.8)。在同一时期内,CD4 最低点从中位数 166 个细胞/mm(IQR:81 至 286)增加到 298 个细胞/mm(IQR:151 至 501)。在最终调整模型中,与 2006 年之前诊断的参与者相比,每个后续 WHO 指南时代诊断的参与者的 ART 起始率均有所增加。与 CD4 最低点<200 个细胞/mm 相比,CD4 最低点≥500 个细胞/mm 与 ART 起始率较低独立相关(HR:0.32;95%CI:0.28 至 0.37)。与 18 至 29 岁相比,诊断时年龄>50 岁与 ART 起始时间较短独立相关(HR:1.38;95%CI:1.19 至 1.61)。
与不断变化的指南一致,诊断和开始 ART 之间的时间间隔随着时间的推移而缩短。尽管如此,许多 HIV 感染者开始治疗时 CD4 较低,这突显了需要在提高即时 ART 获得的同时尽早诊断 HIV。