Fandler-Höfler S, Heschl S, Kneihsl M, Argüelles-Delgado P, Niederkorn K, Pichler A, Deutschmann H, Fazekas F, Berghold A, Enzinger C, Gattringer T
Department of Neurology, Medical University of Graz, Graz, Austria.
Department of Anaesthesiology and Intensive Care Medicine, Medical University of Graz, Graz, Austria.
Eur J Neurol. 2020 May;27(5):849-855. doi: 10.1111/ene.14178. Epub 2020 Mar 17.
The aim was to investigate the clinical impact of the duration of artificial ventilation in stroke patients receiving mechanical thrombectomy (MT) under general anaesthesia.
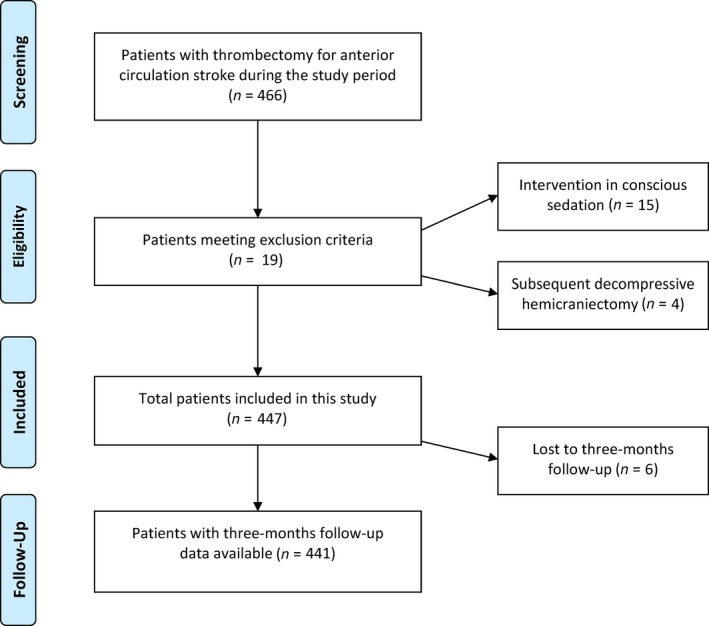
All consecutive ischaemic stroke patients who had been treated at our centre with MT for anterior circulation large vessel occlusion under general anaesthesia were identified over an 8-year period. Ventilation time was analysed as a continuous variable and patients were grouped into extubation within 6 h ('early'), 6-24 h ('delayed') and >24 h ('late'). Favourable outcome was defined as modified Rankin Scale scores of 0-2 at 3 months post-stroke. Pneumonia rate and reasons for prolonged ventilation were also assessed.
Amongst 447 MT patients (mean age 69.1 ± 13.3 years, 50.1% female), the median ventilation time was 3 h. 188 (42.6%) patients had a favourable 3-month outcome, which correlated with shorter ventilation time (Spearman's rho 0.39, P < 0.001). In patients extubated within 24 h, early compared to delayed extubation was associated with improved outcome (odds ratio 2.40, 95% confidence interval 1.53-3.76, P < 0.001). This was confirmed in multivariable analysis (P = 0.01). A longer ventilation time was associated with a higher rate of pneumonia during neurointensive care unit/stroke unit stay (early/delayed/late extubation: 9.6%/20.6%/27.7%, P < 0.01). Whilst stroke-associated complications represented the most common reasons for late extubation (>24 h), delayed extubation (6-24 h) was associated with admission outside of core working hours (P < 0.001).
Prolonged ventilation time after stroke thrombectomy independently predicts unfavourable outcome at 3 months and is associated with increased pneumonia rates. Therefore, extubation should be performed as early as safely possible.
本研究旨在探讨全身麻醉下行机械取栓术(MT)的卒中患者人工通气时长的临床影响。
回顾性分析我院8年间连续收治的在全身麻醉下接受MT治疗前循环大血管闭塞的缺血性卒中患者。将通气时间作为连续变量进行分析,并将患者分为在6小时内拔管(“早期”)、6 - 24小时拔管(“延迟”)和超过24小时拔管(“晚期”)三组。良好预后定义为卒中后3个月改良Rankin量表评分为0 - 2分。同时评估肺炎发生率及通气时间延长的原因。
447例MT患者(平均年龄69.1±13.3岁,女性占50.1%)中,通气时间中位数为3小时。188例(42.6%)患者在3个月时有良好预后,这与较短的通气时间相关(Spearman秩相关系数为0.39,P < 0.001)。在24小时内拔管的患者中,与延迟拔管相比,早期拔管与更好的预后相关(比值比为2.40,95%置信区间为1.53 - 3.76,P < 0.001)。多变量分析证实了这一点(P = 0.01)。在神经重症监护病房/卒中单元住院期间,通气时间越长,肺炎发生率越高(早期/延迟/晚期拔管:9.6%/20.6%/27.7%,P < 0.01)。虽然与卒中相关的并发症是晚期拔管(超过24小时)最常见的原因,但延迟拔管(6 - 24小时)与非核心工作时间入院有关(P < 0.001)。
卒中取栓术后通气时间延长独立预测3个月时预后不良,并与肺炎发生率增加相关。因此,应在安全的前提下尽早拔管。