Developmental Neurosciences, Great Ormond Street Institute of Child Health, University College London, London, UK.
School of Biomedical Engineering & Imaging Sciences, St Thomas' Hospital, King's College London, London, UK.
Epilepsia. 2020 Mar;61(3):433-444. doi: 10.1111/epi.16451. Epub 2020 Feb 17.
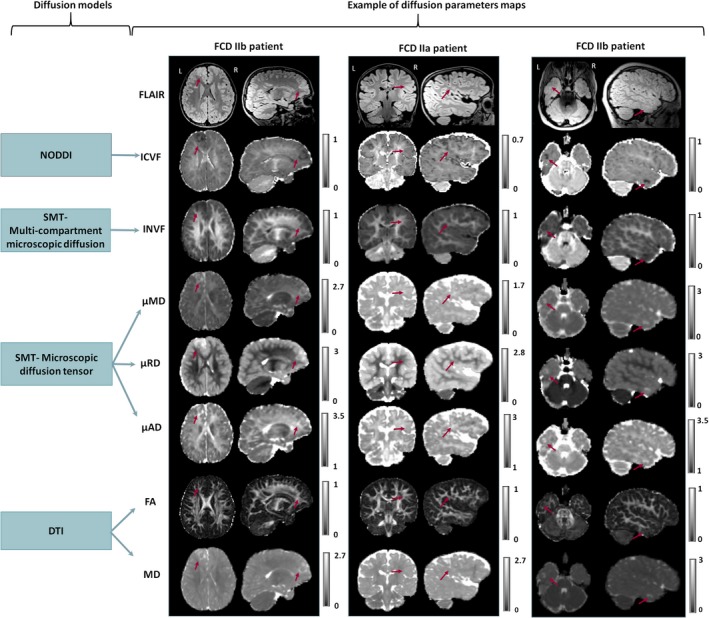
Focal cortical dysplasia (FCD) lesion detection and subtyping remain challenging on conventional MRI. New diffusion models such as the spherical mean technique (SMT) and neurite orientation dispersion and density imaging (NODDI) provide measurements that potentially produce more specific maps of abnormal tissue microstructure. This study aims to assess the SMT and NODDI maps for computational and radiological lesion characterization compared to standard fractional anisotropy (FA) and mean diffusivity (MD).
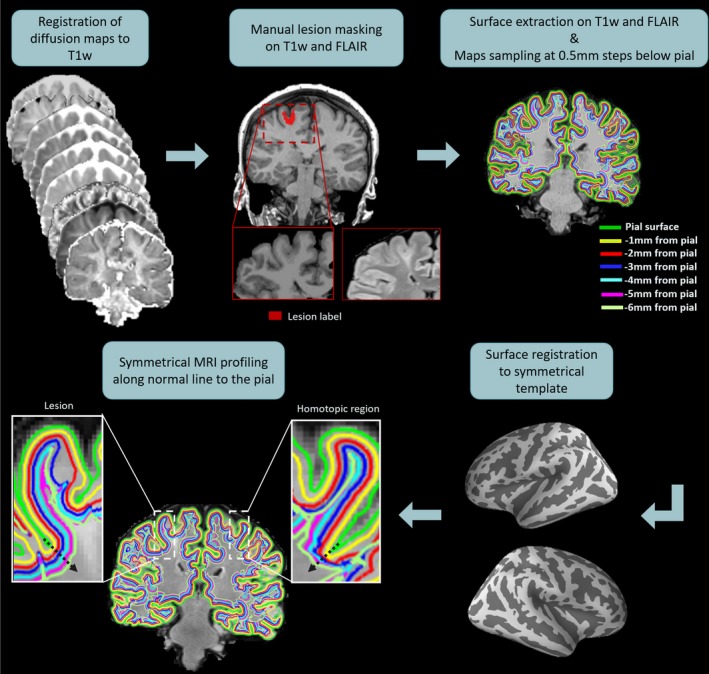
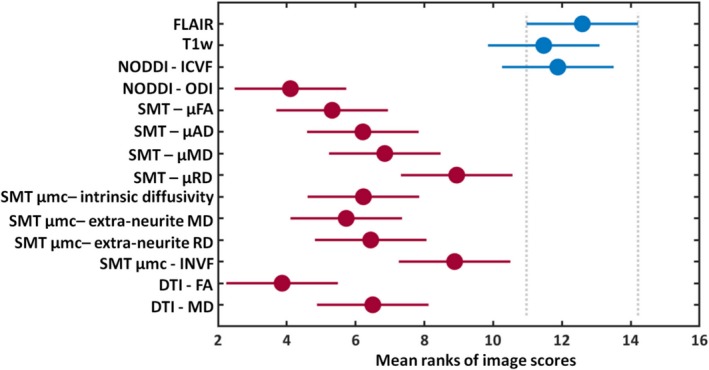
SMT, NODDI, FA, and MD maps were calculated for 33 pediatric patients with suspected FCD (18 histologically confirmed). Two neuroradiologists scored lesion visibility on clinical images and diffusion maps. Signal profile changes within lesions and homologous regions were quantified using a surface-based approach. Diffusion parameter changes at multiple cortical depths were statistically compared between FCD type IIa and type IIb.
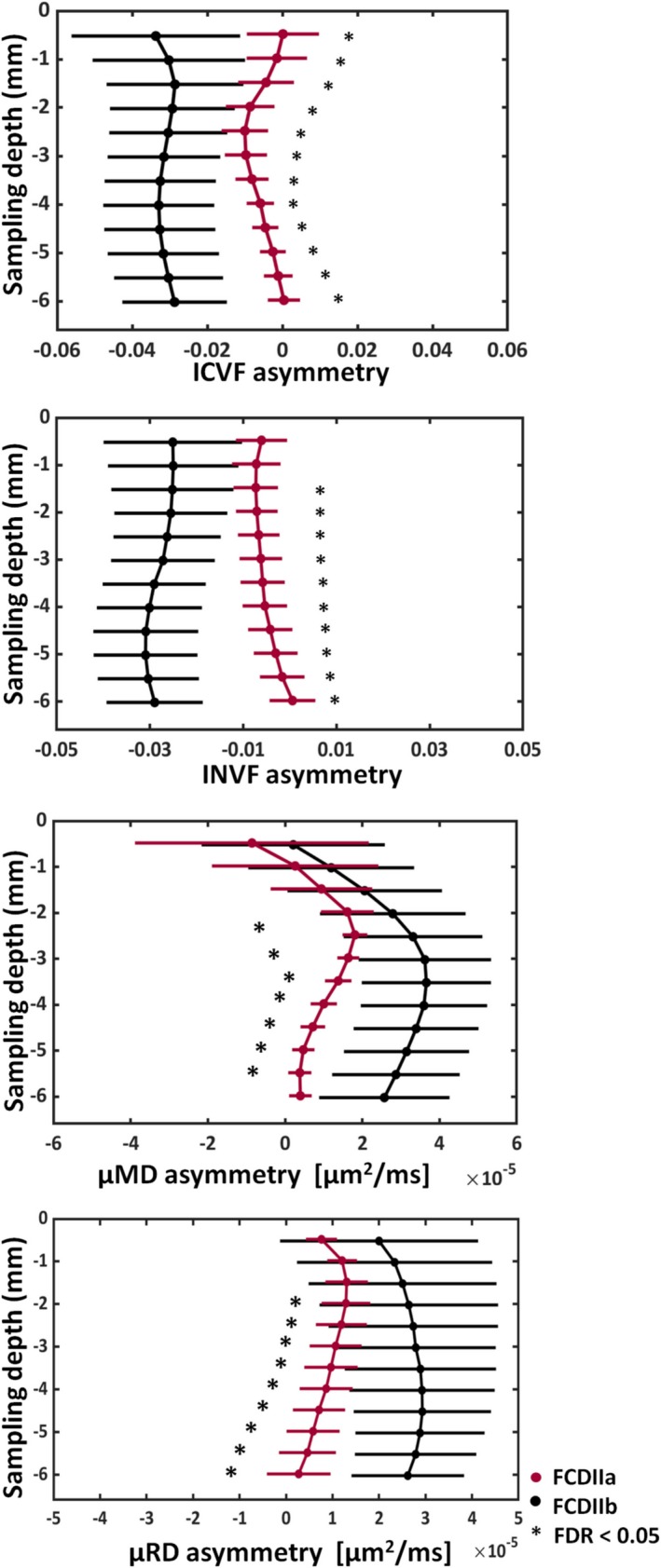
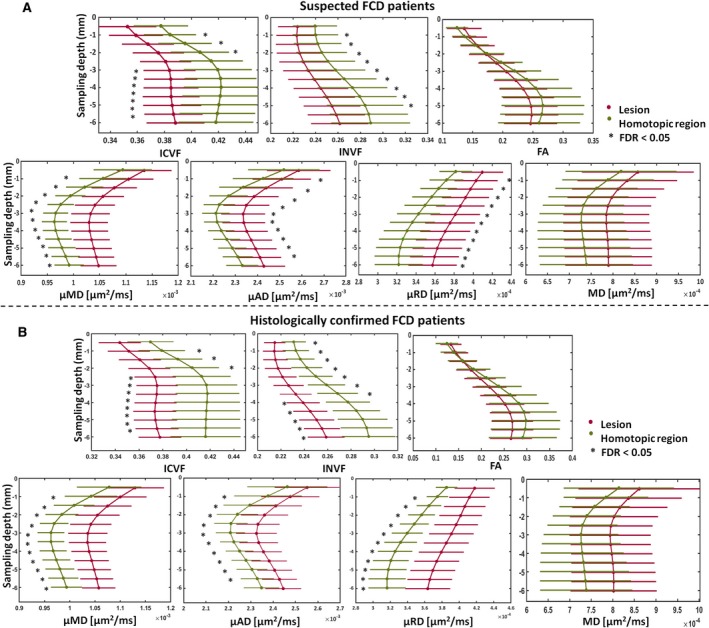
Compared to fluid-attenuated inversion recovery (FLAIR) or T1-weighted imaging, lesions conspicuity on NODDI intracellular volume fraction (ICVF) maps was better/equal/worse in 5/14/14 patients, respectively, while on SMT intra-neurite volume fraction (INVF) in 3/3/27. Compared to FA or MD, lesion conspicuity on the ICVF was better/equal/worse in 27/4/2, while on the INVF in 20/7/6. Quantitative signal profiling demonstrated significant ICVF and INVF reductions in the lesions, whereas SMT microscopic mean, radial, and axial diffusivities were significantly increased. FCD type IIb exhibited greater changes than FCD type IIa. No changes were detected on FA or MD profiles.
FCD lesion-specific signal changes were found in ICVF and INVF but not in FA and MD maps. ICVF and INVF showed greater contrast than FLAIR in some cases and had consistent signal changes specific to FCD, suggesting that they could improve current presurgical pediatric epilepsy imaging protocols and can provide features useful for automated lesion detection.
在常规 MRI 上,局灶性皮质发育不良(FCD)病灶的检测和分型仍然具有挑战性。新的扩散模型,如球均值技术(SMT)和神经丝取向分散和密度成像(NODDI),提供了潜在的更特异的异常组织微观结构的测量值。本研究旨在评估 SMT 和 NODDI 图谱在计算和放射学病变特征方面与标准各向异性分数(FA)和平均弥散度(MD)的比较。
为 33 名疑似 FCD 的儿科患者(18 例经组织学证实)计算 SMT、NODDI、FA 和 MD 图。两位神经放射科医生对临床图像和弥散图上的病变可见性进行评分。使用基于表面的方法量化病变内和同源区域的信号轮廓变化。在 FCD IIa 型和 IIb 型之间,在多个皮质深度比较扩散参数的变化。
与液体衰减反转恢复(FLAIR)或 T1 加权成像相比,NODDI 细胞内容积分数(ICVF)图上的病变显影在 5/14/14 例中分别更好/相等/更差,而在 SMT 内神经丝容积分数(INVF)图上分别为 3/3/27。与 FA 或 MD 相比,在 ICVF 上病变显影在 27/4/2 例中更好/相等/更差,而在 INVF 上在 20/7/6 例中更好/相等/更差。定量信号分析显示,病变的 ICVF 和 INVF 显著降低,而 SMT 微观平均、径向和轴向弥散度显著增加。FCD IIb 型比 FCD IIa 型的变化更大。在 FA 或 MD 图谱上未检测到变化。
在 ICVF 和 INVF 中发现了 FCD 病变特异性信号变化,但在 FA 和 MD 图谱中没有发现。在某些情况下,ICVF 和 INVF 比 FLAIR 具有更大的对比度,并且具有与 FCD 特异性的一致信号变化,这表明它们可以改善当前儿科癫痫术前成像方案,并能提供有助于自动病变检测的特征。