Department of Diagnostic and Interventional Neuroradiology, University Medical Center Hamburg-Eppendorf, Haus Ost 22 (O 22), Martinistr. 52, 20246, Hamburg, Germany.
Department of Neurology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany.
Clin Neuroradiol. 2021 Mar;31(1):197-205. doi: 10.1007/s00062-020-00880-8. Epub 2020 Feb 17.
In acute large vessel occlusions, endovascular therapy (EVT) achieves flow restoration in the majority of cases; however, EVT fails to achieve sufficient reperfusion in a substantial minority of patients. This study aimed to identify predictors of failed reperfusion.
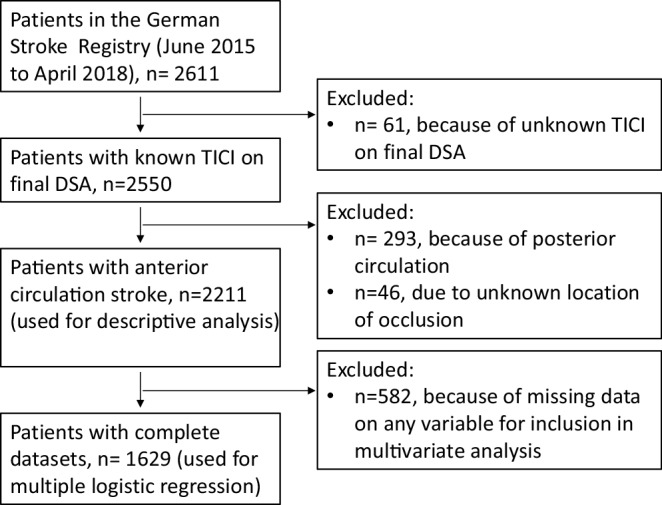
In this study 2211 patients from the German Stroke Registry who received EVT for anterior circulation stroke were retrospectively analyzed. Failure of reperfusion was defined as thrombolysis in cerebral infarction (TICI) grades 0/1/2a, and sufficient reperfusion as TICI 2b/3. In 1629 patients with complete datasets, associations between failure of reperfusion and baseline clinical data, comorbidities, location of occlusion, and procedural data were assessed with multiple logistic regression.
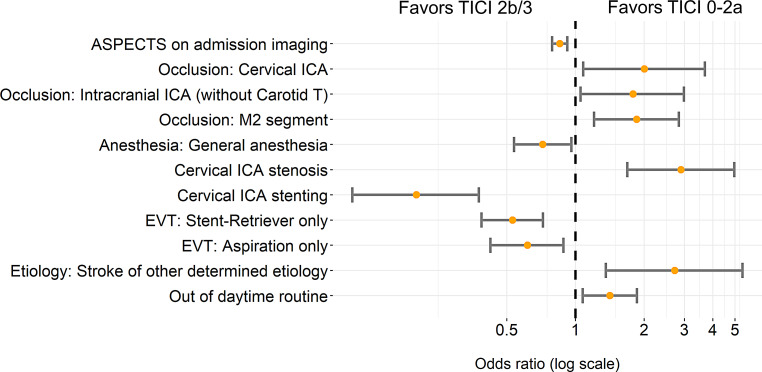
Failure of reperfusion occurred in 371 patients (16.8%) and was associated with the following locations of occlusion: cervical internal carotid artery (ICA, adjusted odds ratio, OR 2.01, 95% confidence interval, CI 1.08-3.69), intracranial ICA without carotid T occlusion (adjusted OR 1.79, 95% CI 1.05-2.98), and M2 segment (adjusted OR 1.86, 95% CI 1.21-2.84). Failed reperfusion was also associated with cervical ICA stenosis (>70% stenosis, adjusted OR 2.90, 95% CI 1.69-4.97), stroke of other determined etiology by TOAST (Trial of ORG 10172 in acute stroke treatment) criteria (e.g. nonatherosclerotic vasculopathies, adjusted OR 2.73, 95% CI 1.36-5.39), and treatment given outside the usual working hours (adjusted OR 1.41, 95% CI 1.07-1.86). Successful reperfusion was associated with higher Alberta stroke program early CT score (ASPECTS) on initial imaging (adjusted OR 0.85, 95% CI 0.79-0.92), treatment with the patient under general anesthesia (adjusted OR 0.72, 95% CI 0.54-0.96), and concomitant ICA stenting in patients with ICA stenosis (adjusted OR 0.20, 95% CI 0.11-0.38).
Several factors are associated with failure of reperfusion, most notably occlusions of the proximal ICA and low ASPECTS on admission. Conversely, stent placement in the proximal ICA was associated with reperfusion success.
在急性大血管闭塞中,血管内治疗(EVT)可使大多数病例恢复血流;然而,EVT 未能使相当一部分患者实现充分再灌注。本研究旨在确定再灌注失败的预测因素。
本研究回顾性分析了德国卒中登记处 2211 例接受前循环卒中 EVT 治疗的患者。再灌注失败定义为血栓溶解治疗脑梗死(TICI)分级 0/1/2a,充分再灌注定义为 TICI 2b/3。在 1629 例具有完整数据集的患者中,采用多因素逻辑回归评估再灌注失败与基线临床数据、合并症、闭塞部位和手术数据之间的关系。
371 例(16.8%)患者发生再灌注失败,与以下闭塞部位相关:颈内动脉(ICA)(校正比值比,OR 2.01,95%置信区间,CI 1.08-3.69)、无颈内动脉 T 闭塞的颅内 ICA(校正 OR 1.79,95%CI 1.05-2.98)和 M2 段(校正 OR 1.86,95%CI 1.21-2.84)。再灌注失败也与颈内动脉狭窄(>70%狭窄,校正 OR 2.90,95%CI 1.69-4.97)、TOAST(急性卒中治疗 ORG 10172 试验)标准确定的其他确定病因的卒中(如非动脉粥样硬化性血管病,校正 OR 2.73,95%CI 1.36-5.39)以及在常规工作时间之外进行治疗(校正 OR 1.41,95%CI 1.07-1.86)有关。成功再灌注与初始影像学检查时较高的阿尔伯塔卒中项目早期 CT 评分(ASPECTS)(校正 OR 0.85,95%CI 0.79-0.92)、全身麻醉下治疗(校正 OR 0.72,95%CI 0.54-0.96)和颈内动脉狭窄患者同时行颈内动脉支架置入(校正 OR 0.20,95%CI 0.11-0.38)有关。
几个因素与再灌注失败相关,最显著的是近端 ICA 闭塞和入院时 ASPECTS 评分较低。相反,近端 ICA 支架置入与再灌注成功相关。