Department of Biochemistry and Molecular Genetics, Hospital Clínic, Barcelona, Spain.
Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain.
Ann Lab Med. 2020 Jul;40(4):285-296. doi: 10.3343/alm.2020.40.4.285.
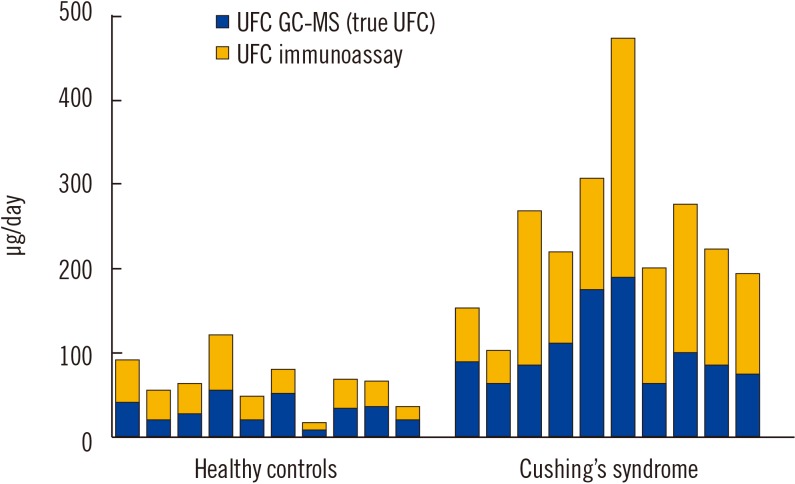
Determination of cortisol levels in the urine (24 hours urine free cortisol), saliva (late-night), or serum (total cortisol after dexamethasone suppression) is recommended to screen for Cushing's syndrome (CS). This review focuses on the differences between the frequently used cortisol-antibody immunoassay-based methods and the highly specific mass-spectrometry-based methods that are progressively being employed in clinical laboratories for CS screening. The particular characteristics of cortisol metabolism and the lack of specificity of the immunoassays cause marked differences between both methods that are in turn highly dependent on the biological matrix, in which the cortisol is measured. Understanding the origin of these differences is essential for the interpretation of these results. Although cross-reactivity with endogenous steroids leads to grossly inaccurate results of immunoassay measurements of cortisol in the saliva and urine, preliminary evidence suggests that the clinical sensitivity of CS screening using immunoassays may be similar to CS screening using mass spectrometry. However, mass spectrometry offers more accurate results and considerably reduced variation across laboratories, while avoiding false-positive results. Moreover, mass spectrometry can overcome some common diagnostic challenges, such as identification of exogenous corticosteroids or simultaneous assessment of appropriate dexamethasone levels in suppression tests. Further, comprehensive mass spectrometry-based profiling of several steroid metabolites may be useful for discriminating among different subtypes of CS. Finally, this review discusses the main preanalytical factors that could cause variations in cortisol measurements and their influence on the reliability of the results.
建议测定尿液(24 小时尿游离皮质醇)、唾液(深夜)或血清(地塞米松抑制后总皮质醇)中的皮质醇水平,以筛查库欣综合征(CS)。本综述重点介绍了经常使用的基于皮质醇抗体免疫测定法的方法与高度特异的基于质谱的方法之间的差异,这些方法正逐渐应用于临床实验室进行 CS 筛查。皮质醇代谢的特殊特征和免疫测定法的非特异性导致这两种方法之间存在明显差异,而这些差异又高度依赖于皮质醇被测量的生物基质。了解这些差异的来源对于解释这些结果至关重要。尽管内源性类固醇的交叉反应导致免疫测定法测量唾液和尿液中皮质醇的结果严重不准确,但初步证据表明,使用免疫测定法进行 CS 筛查的临床敏感性可能与使用质谱法进行 CS 筛查相似。然而,质谱法提供了更准确的结果和实验室间的差异大大减少,同时避免了假阳性结果。此外,质谱法可以克服一些常见的诊断挑战,例如鉴定外源性皮质激素或同时评估抑制试验中适当的地塞米松水平。此外,基于全面的质谱的几种类固醇代谢物的分析可能有助于区分不同类型的 CS。最后,本综述讨论了可能导致皮质醇测量值变化的主要分析前因素及其对结果可靠性的影响。