Department of Infectious Disease Epidemiology, Imperial College London, London, UK.
Department of Medicine, Section of Paediatrics, Imperial College London, London, UK.
BMC Pediatr. 2020 Feb 18;20(1):75. doi: 10.1186/s12887-020-1976-7.
Clostridium perfringens forms part of the human gut microbiota and has been associated with life-threatening necrotising enterocolitis (NEC) in premature infants. Whether specific toxigenic strains are responsible is unknown, as is the extent of diversity of strains in healthy premature babies. We investigated the C. perfringens carrier status of premature infants in the neonatal intensive care unit, factors influence this status, and the toxic potential of the strains.
C. perfringens was isolated by culture from faecal samples from 333 infants and their toxin gene profiles analysed by PCR. A survival analysis was used to identify factors affecting probability of carriage. Competitive growth experiments were used to explore the results of the survival analysis.
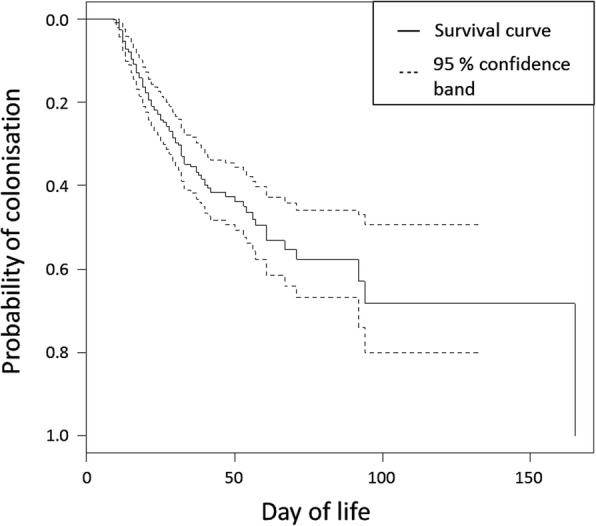
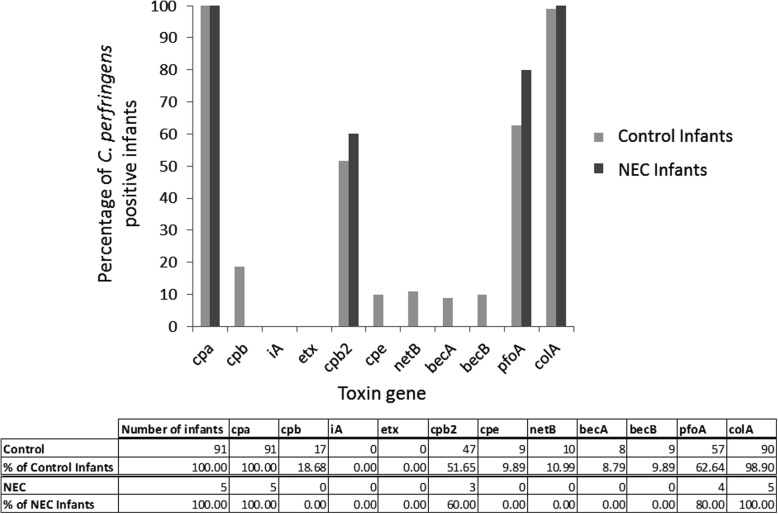
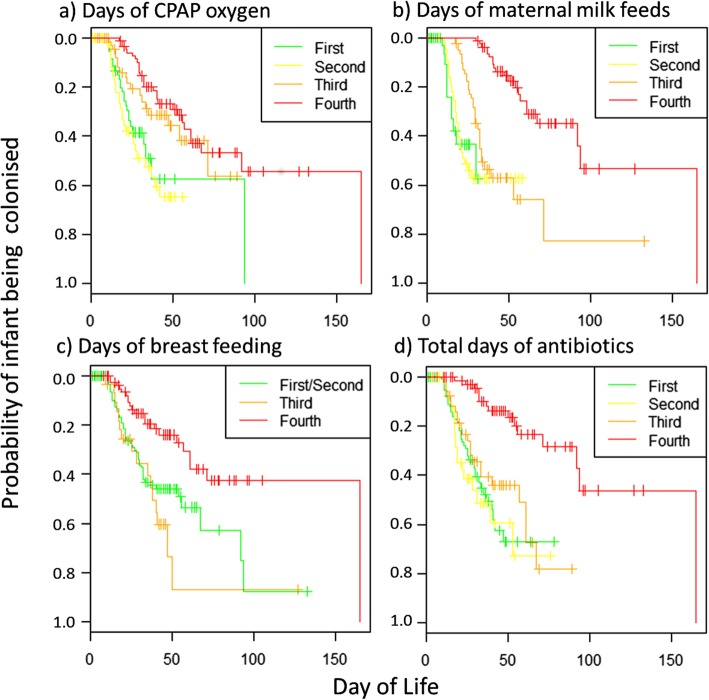
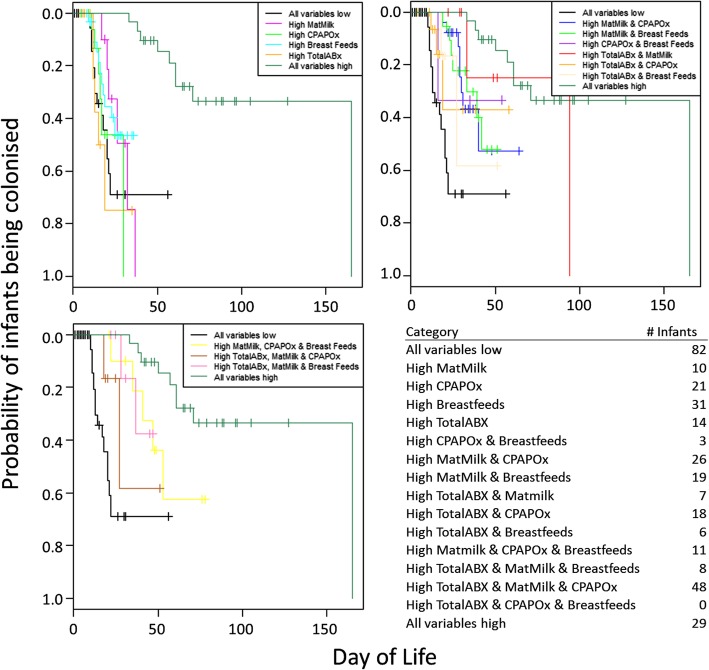
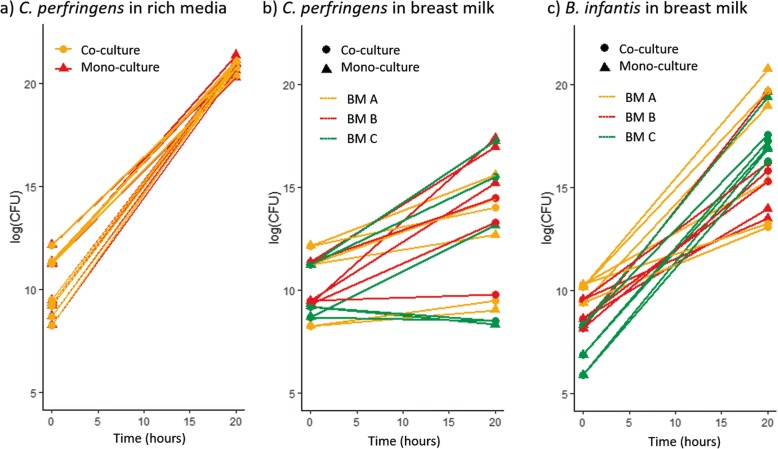
29.4% of infants were colonized with C. perfringens before they left hospital. Three factors were inversely associated with probability of carriage: increased duration of maternal milk feeds, CPAP oxygen treatment and antibiotic treatment. C. perfringens grew poorly in breast milk and was significantly outperformed by Bifidobacterium infantis, whether grown together or separately. Toxin gene screening revealed that infants carried isolates positive for collagenase, perfringolysin O, beta 2, beta, becA/B, netB and enterotoxin toxin genes, yet none were observed to be associated with the development of NEC.
Approximately a third of preterm infants are colonised 3 weeks after birth with toxin gene-carrying C. perfringens. We speculate that increased maternal breast milk, oxygen and antibiotic treatment creates an environment in the gut hostile to growth of C. perfringens. Whilst potentially toxigenic C. perfringens isolates were frequent, no toxin type was associated with NEC.
clinicaltrials.gov NCT01102738, registered 13th April 2010.
产气荚膜梭菌是人类肠道微生物群的一部分,与早产儿致命性坏死性小肠结肠炎(NEC)有关。是否特定的产毒菌株是致病原因尚不清楚,健康早产儿中产气荚膜梭菌菌株的多样性程度也不清楚。我们调查了新生儿重症监护病房中早产儿的产气荚膜梭菌携带状态、影响这种状态的因素以及菌株的毒性潜力。
通过培养从 333 名婴儿的粪便样本中分离产气荚膜梭菌,并通过 PCR 分析其毒素基因谱。生存分析用于确定影响携带概率的因素。竞争生长实验用于探索生存分析的结果。
29.4%的婴儿在离开医院前被产气荚膜梭菌定植。有三个因素与携带概率呈负相关:母亲母乳喂养时间延长、CPAP 氧疗和抗生素治疗。产气荚膜梭菌在母乳中生长不良,无论是与婴儿双歧杆菌一起生长还是单独生长,都明显优于后者。毒素基因筛查显示,婴儿携带的分离株对胶原酶、产气荚膜梭菌α毒素、β2、β、becA/B、netB 和肠毒素基因呈阳性,但均未发现与 NEC 的发展有关。
大约三分之一的早产儿在出生后 3 周被产毒基因携带的产气荚膜梭菌定植。我们推测,增加的母亲母乳喂养、氧气和抗生素治疗会使肠道环境不利于产气荚膜梭菌的生长。虽然频繁出现潜在产毒的产气荚膜梭菌分离株,但没有一种毒素类型与 NEC 有关。
clinicaltrials.gov NCT01102738,于 2010 年 4 月 13 日注册。