Eastern Virginia Medical School, 700 West Olney Ave, Norfolk, VA, USA.
Department of Orthopaedic Surgery, Wright State University, Dayton, OH, USA.
J Orthop Surg Res. 2020 Feb 18;15(1):56. doi: 10.1186/s13018-020-1581-3.
Biceps tenotomy and tenodesis are surgical treatments for pathology of the proximal tendon of the long head of the biceps. There is debate over which procedure provides better patient outcomes.
Compare patient-reported outcomes and satisfaction between biceps tenotomy and tenodesis.
This retrospective cohort study including all patients undergoing arthroscopic biceps tenodesis or tenotomy as part of more extensive shoulder surgery with a single surgeon. Concomitant procedures included rotator cuff repair, subacromial decompression, acromioclavicular joint resection, and debridement. Patients 36-81 years old were contacted by phone at > 2-year post-operatively to complete a biceps-specific outcome questionnaire. Subject decision not to participate was the sole exclusion criterion. Satisfaction scores and frequencies of potential biceps-related downsides (biceps cramping/spasms, biceps pain, shoulder pain, weakness, cosmetic deformity) were analyzed for the effects of procedure, sex, and age.
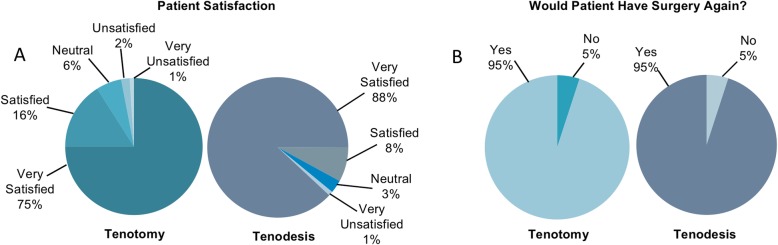
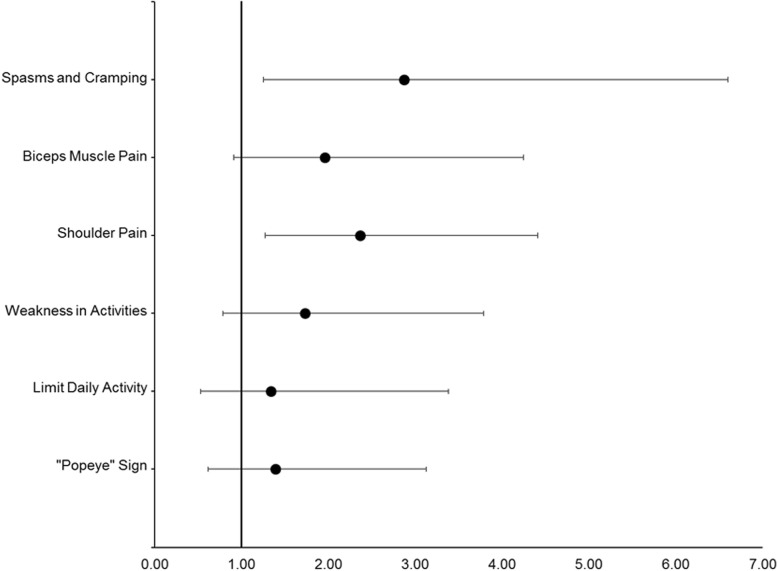
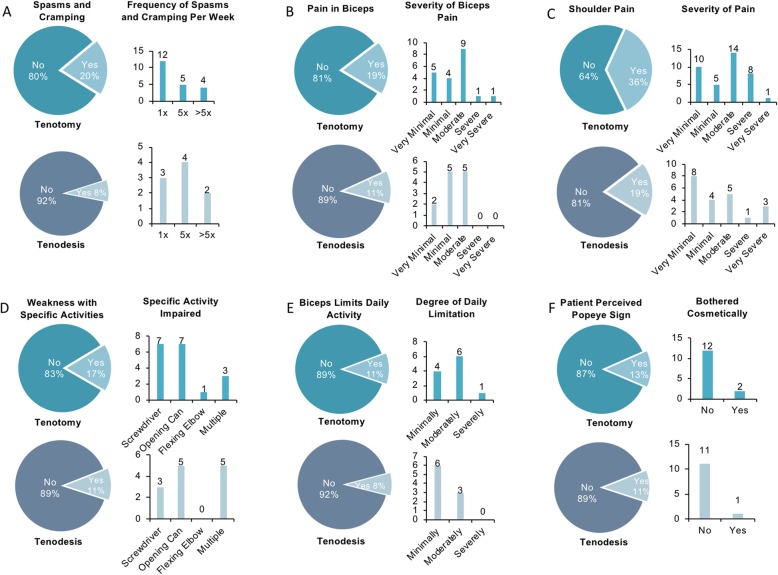
Satisfaction score distributions were similar between patients with tenodesis and patients with tenotomy (χ = 8.34, P = 0.08), although slightly more patients with tenodesis than patients with tenotomy reported being satisfied or very satisfied (96% versus 91%). Perceived downsides occurred more frequently among patients with tenotomy than in patients with tenodesis: 59% of patients with tenotomy reported ≥ 1 downside, versus 37% of patients with tenodesis (P < 0.01). In patients reporting ≥ 1 downside, distributions of total downsides differed between procedures (χ = 10.04, P = 0.04): patients with tenotomy were more likely to report multiple concurrent downsides than were patients with tenodesis (31% versus 16%). Each individual downside tended to be reported as present by a greater proportion of patients with tenotomy than patients with tenodesis. Sex had no effect on satisfaction or downsides, but there was a trend for older patients to report higher satisfaction and fewer downsides.
Biceps tenotomy and tenodesis are both viable treatments for proximal biceps tendon pathology, yielding high patient satisfaction. There were trends toward greater satisfaction and fewer problems in patients with tenodesis. Still, younger patients with tenodesis did report perceived downsides. Alternatively, older patients tended to be more satisfied with both procedures overall. Regardless of procedure, most patients receiving either tenotomy or tenodesis would undergo their respective surgery again.
Level III evidence, retrospective comparative cohort study.
肱二头肌肌腱切断术和肌腱固定术是治疗肱二头肌长头近端肌腱病变的手术治疗方法。对于哪种手术方法能提供更好的患者预后,存在争议。
比较肱二头肌肌腱切断术和肌腱固定术的患者报告结局和满意度。
本回顾性队列研究纳入了所有接受关节镜下肱二头肌肌腱固定术或肌腱切断术的患者,这些患者均为同一外科医生行更广泛的肩部手术的一部分。同时进行的手术包括肩袖修复、肩峰下减压、肩锁关节切除和清创术。术后 > 2 年,通过电话联系年龄在 36-81 岁之间的患者,完成肱二头肌特定的结局问卷。患者决定不参与是唯一的排除标准。分析手术、性别和年龄对满意度评分和潜在肱二头肌相关不良影响(肱二头肌痉挛/抽搐、肱二头肌疼痛、肩部疼痛、无力、美容畸形)的频率的影响。
肌腱固定术和肌腱切断术患者的满意度评分分布相似(χ²= 8.34,P = 0.08),尽管肌腱固定术患者报告满意或非常满意的比例略高于肌腱切断术患者(96%比 91%)。与肌腱固定术患者相比,肌腱切断术患者更常报告存在≥1 种不良影响:59%的肌腱切断术患者报告存在≥1 种不良影响,而肌腱固定术患者为 37%(P < 0.01)。在报告存在≥1 种不良影响的患者中,两种手术的总不良影响分布不同(χ²= 10.04,P = 0.04):肌腱切断术患者更有可能报告多种同时存在的不良影响,而肌腱固定术患者则较少(31%比 16%)。与肌腱固定术患者相比,更多的肌腱切断术患者报告存在各种不良影响。性别对满意度或不良影响无影响,但年龄较大的患者报告满意度较高,不良影响较少。
肱二头肌肌腱切断术和肌腱固定术都是治疗肱二头肌长头近端肌腱病变的可行方法,患者满意度高。肌腱固定术患者的满意度更高,不良影响更少,但年轻的肌腱固定术患者仍报告存在不良影响。相比之下,年龄较大的患者总体上对两种手术都更满意。无论采用哪种手术,接受肌腱切断术或肌腱固定术的大多数患者都会再次接受各自的手术。
III 级证据,回顾性比较队列研究。